

Randomized Comparison of Endoscopic Cartilage-Perichondrium Sandwich Technique Verses Underlay Technique for Large Tympanic Membrane Perforations
- PMID: 40259768
- PMCID: PMC12034960
- DOI: 10.1177/19160216251333748
Randomized Comparison of Endoscopic Cartilage-Perichondrium Sandwich Technique Verses Underlay Technique for Large Tympanic Membrane Perforations
Abstract
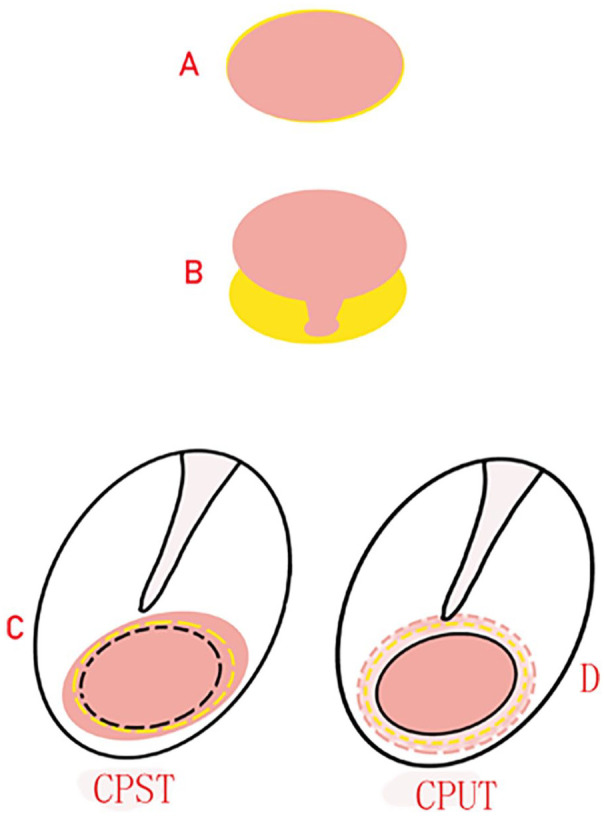
ImportantTrimming perforation margins is the basic procedure for any myringoplasties; however, to date, little literature has been reported on the effect of no trimming perforation margins on sandwich graft tympanoplasty.ObjectiveThe objective of this study was to compare the graft success rate, hearing improvement, and complications of endoscopic cartilage-perichondrium Sandwich technique (CPST) and cartilage-perichondrium underlay technique (CPUT) for repairing chronic large perforations.Study DesignProspective randomized controlled trial.SettingTertiary referral center.Participants and InterventionOne hundred two patients with chronic large perforations with 50% to 75% of tympanic membrane (TM) were recruited and randomly allocated to CPST (n = 51) and CPUT (n = 51), raising tympanomeatal flap and trimming perforation margins were not performed in both techniques.Main Outcome MeasurersThe graft success rate, air-bone gap (ABG) gain, operation time, and postoperative complications were evaluated at 12 months.ResultsAll the patients complete 12 months follow-up. The mean operation time was 30.6 ± 3.7 minutes in the CPST group and 29.8 ± 6.1 minutes in the CPUT group (P = .751).The graft success rate was 92.2% in the CPST group and 96.1% in the CPUT group (P = .979). Endoscopic examination revealed the perichondrial flap gradually became scab in the CPST group, 70.6% patients had the absence of typical cone-shaped TM. However, no scab was seen on the surface of graft, and all the patients had cone-shaped TM in the CPUT group. The ABG gain wasn't significantly different (12.9 ± 3.3 dB vs 13.1 ± 1.7 dB, P = .689).The successful surgery was 94.1% in the CPST group and 96.1% in the CPUT group, the difference wasn't significant among the 2 groups (P = .932). In addition, no procedure-related complications and no graft cholesteatoma were found in both groups during the follow-up period.Conclusions and RelevanceThe operation time, 12 months graft success rate, hearing improvement were comparable between CPST and CPUT for repairing large perforation, although raising tympanomeatal flap and trimming the perforation margins were not performed in both techniques.
Keywords: Sandwich graft; cartilage graft; endoscope; myringoplasty; perichondrium tucking technique; underlay graft.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




Similar articles
-
Comparison of long-term outcome of two endoscopic transtympanic myringoplasty without tympanomeatal flap elevating for repairing large chronic perforations.Eur Arch Otorhinolaryngol. 2022 May;279(5):2293-2301. doi: 10.1007/s00405-021-06913-3. Epub 2021 May 30. Eur Arch Otorhinolaryngol. 2022. PMID: 34052865
-
Comparative study of endoscopic underlay myringoplasty with or without tucking of the attached perichondrium graft when repairing large central dry perforations.Am J Otolaryngol. 2024 Nov-Dec;45(6):104471. doi: 10.1016/j.amjoto.2024.104471. Epub 2024 Aug 14. Am J Otolaryngol. 2024. PMID: 39151379 Clinical Trial.
-
Effects of no perforation margin trimming and EAC packing in cartilage underlay myringoplasty for chronic large perforations in children.Int J Pediatr Otorhinolaryngol. 2024 May;180:111956. doi: 10.1016/j.ijporl.2024.111956. Epub 2024 Apr 14. Int J Pediatr Otorhinolaryngol. 2024. PMID: 38657426 Clinical Trial.
-
Endoscopic modified perichondrium-cartilage sandwich graft for repairing chronic subtotal and total perforations.Am J Otolaryngol. 2022 Jan-Feb;43(1):103231. doi: 10.1016/j.amjoto.2021.103231. Epub 2021 Sep 15. Am J Otolaryngol. 2022. PMID: 34537512
-
Full-thickness cartilage graft myringoplasty combined with topical application of bFGF for repair of perforations with extensive epithelialization.Auris Nasus Larynx. 2021 Aug;48(4):601-608. doi: 10.1016/j.anl.2020.11.013. Epub 2020 Nov 27. Auris Nasus Larynx. 2021. PMID: 33257105 Review.
References
-
- Atchariyasathian V, Suwannajak R, Plodpai Y, Pitathawatchai P. A comparison of endoscopic transtympanic myringoplasty and endoscopic type I tympanoplasty for repairing medium- to large-sized tympanic membrane perforation: a randomized clinical trial. Eur Arch Otorhinolaryngol. 2020;277:2199-2207. - PubMed
-
- Berglund M, Suneson P, Florentzson R, et al. Tinnitus and taste disturbances reported after myringoplasty: data from a national quality registry. Laryngoscope. 2019;129:209-215. - PubMed
-
- Farrior JB. Sandwich graft tympanoplasty: experience, results, and complications. Laryngoscope. 1989;99(2):213-217. - PubMed
-
- Lou Z, Lou Z, Jin K, Sun J, Chen Z. Comparison of long-term outcome of two endoscopic transtympanic myringoplasty without tympanomeatal flap elevating for repairing large chronic perforations. Eur Arch Otorhinolaryngol. 2022;279(5):2293-2301. - PubMed
-
- Lou Z. Transcanal endoscopic cartilage and perichondrium graft myringoplasty for large tympanic membrane perforations. Otol Neurotol. 2021;42(8):1172-1176. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
