

Social factors, health policy, and environment: implications for cardiovascular disease across the globe
- PMID: 40259769
- PMCID: PMC12342468
- DOI: 10.1093/eurheartj/ehaf212
Social factors, health policy, and environment: implications for cardiovascular disease across the globe
Abstract
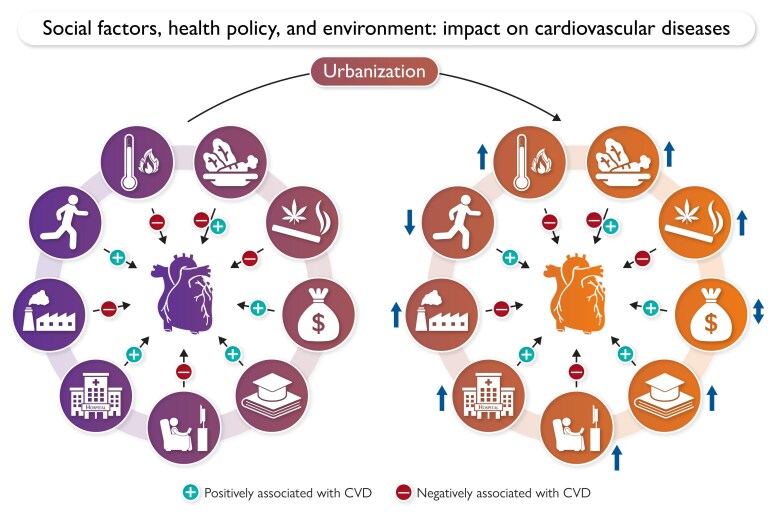
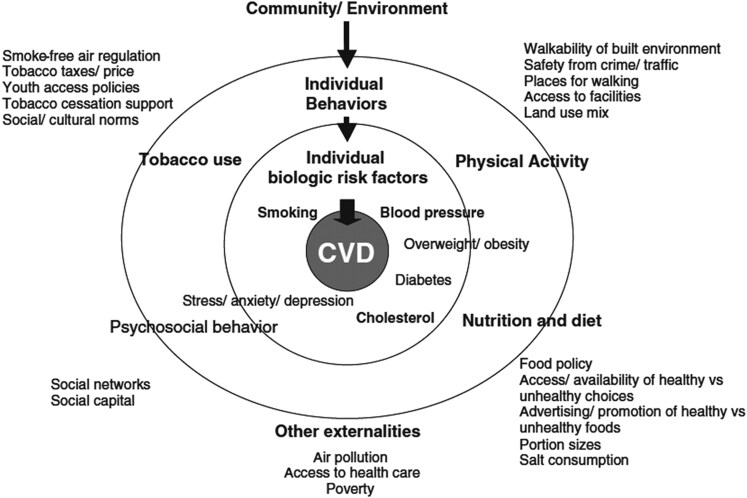
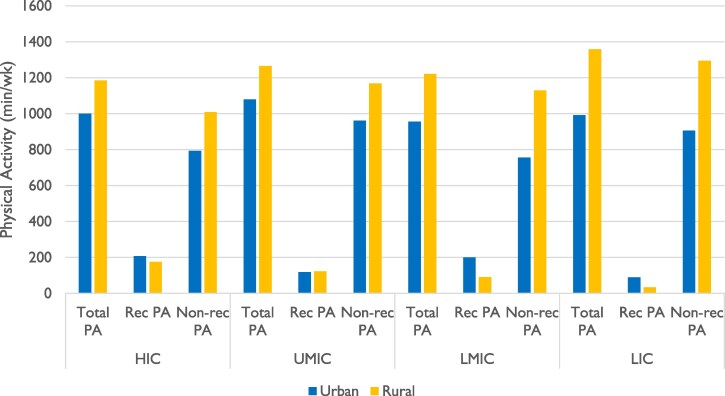
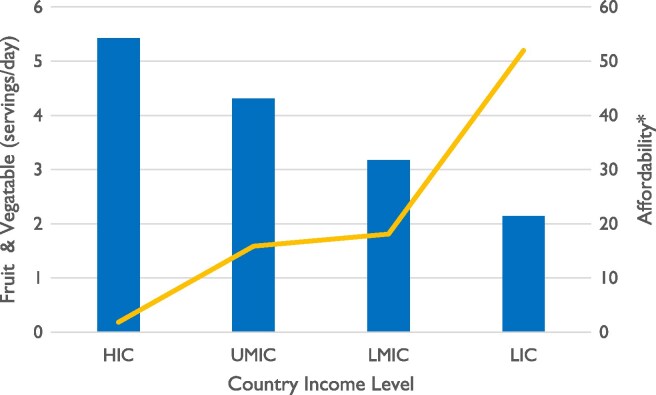
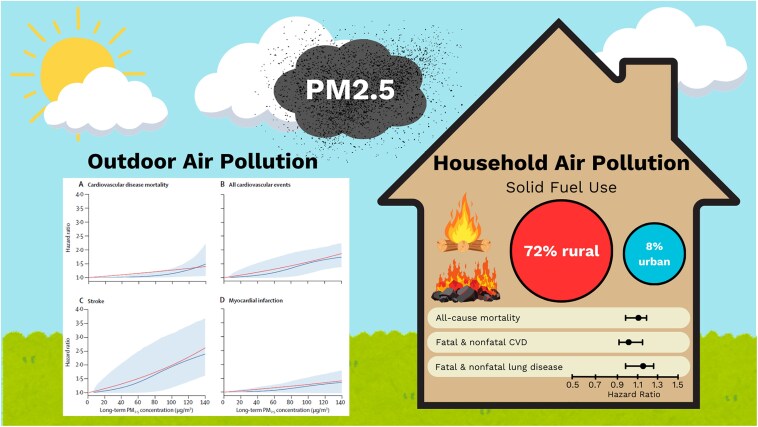
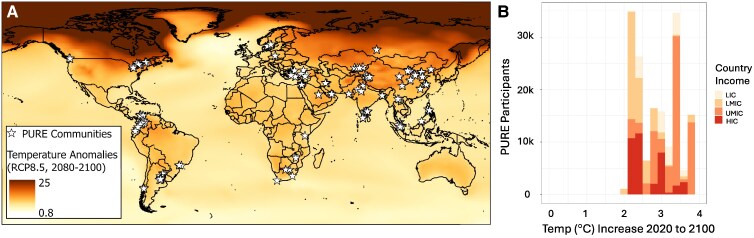
Cardiovascular disease (CVD) is the leading cause of deaths worldwide, with 80% occurring in low- and middle-income countries. These countries are characterized by rapid urbanization, poorly funded health systems, poor access to prevention and treatment strategies, and increasing age and a higher prevalence of chronic disease. Rapid urbanization has contributed to the significant environmental and societal changes affecting daily life habits and cardiovascular health. There is growing awareness that environmental and social exposures and policies can influence CVD directly or through behavioural risk factors. However, much of this knowledge comes from studies in high-income countries and is applied to low- and middle-income countries without evidence to indicate this is appropriate. This state-of-the-art review will present and synthesize key findings from the Prospective Urban Rural Epidemiology study and related studies that have aimed to understand the environmental, social, and policy determinants of cardiovascular health in countries across varying levels of economic development through an urban/rural lens. Emerging from these findings are future policy and research recommendations to accelerate the reduction of the global burden of CVD.
Keywords: Access to care; Cardiovascular disease; Diet; Environment; Physical activity; Pollution; Social determinants.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Practical dietary interventions to prevent cardiovascular disease suitable for implementation in primary care: an ADAPTE-guided systematic review of international clinical guidelines.Int J Behav Nutr Phys Act. 2023 Jul 28;20(1):93. doi: 10.1186/s12966-023-01463-9. Int J Behav Nutr Phys Act. 2023. PMID: 37507692 Free PMC article.
-
The Lived Experience of Autistic Adults in Employment: A Systematic Search and Synthesis.Autism Adulthood. 2024 Dec 2;6(4):495-509. doi: 10.1089/aut.2022.0114. eCollection 2024 Dec. Autism Adulthood. 2024. PMID: 40018061 Review.
-
The Changing Epidemiology of Type 1 Diabetes: A Global Perspective.Diabetes Obes Metab. 2025 Aug;27 Suppl 6(Suppl 6):3-14. doi: 10.1111/dom.16501. Epub 2025 Jun 19. Diabetes Obes Metab. 2025. PMID: 40536127 Free PMC article. Review.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
References
-
- Global Burden of Disease . GBD Compare. https://vizhub.healthdata.org/gbd-compare/ (5 January 2024, date last accessed).
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2197–223. 10.1016/s0140-6736(12)61689-4 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
