

Identification of a Gene Expression Signature to Predict the Risk of Abdominal Aortic Aneurysm in Psoriasis Patients
- PMID: 40260094
- PMCID: PMC12011042
- DOI: 10.2147/CCID.S495890
Identification of a Gene Expression Signature to Predict the Risk of Abdominal Aortic Aneurysm in Psoriasis Patients
Abstract
Background : Psoriasis is an immune-mediated, hereditary condition that presents itself in the skin or joints, or even both. Increasing evidence indicates that psoriasis is connected to an elevated risk of abdominal aortic aneurysm (AAA), owing to their shared inflammatory pathogenesis. Nevertheless, the interplay between psoriasis and AAA lacks sufficient documentation.
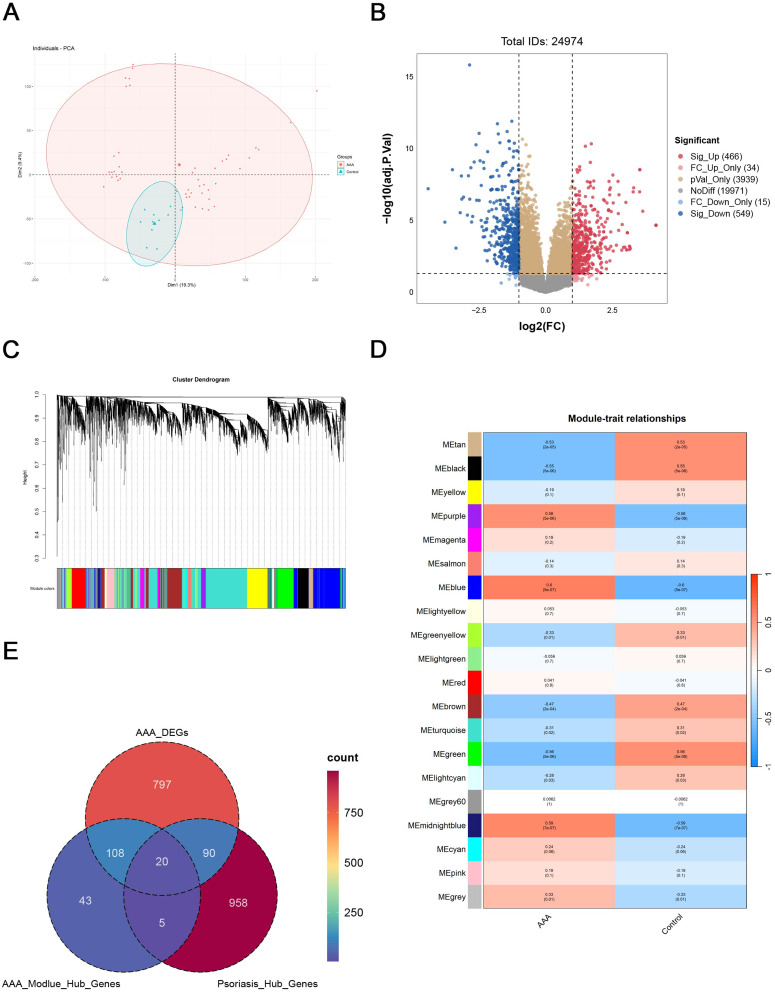
Methods: Through WGCNA and DEGs, psoriasis and AAA phenotype-related genes were identified. Identifying risk genes involved in both psoriasis and AAA involved generating candidate genes by finding the common intersection of hub genes, followed by using LASSO regression. Following this, a nomogram was created to forecast the development of psoriasis alongside AAA, and was then assessed through a ROC curve, DCA, calibration curve, and PR curve. Five algorithms, namely CIBERSORT, ssGSEA, ESTIMATE, MCPcounter, and QuanTIseq, were utilized to assess immune infiltration differences between high and low-risk groups. Simultaneously, we verified the differential gene expression in different tissues.
Results: A total of 1073 psoriasis hub genes and 128 AAA hub genes were generated. A Venn diagram revealed 20 candidate genes that were common to both hub genes of psoriasis and AAA. Of these, six genes (CCR7, CD3D, GBP5, HCLS1, IL7R, and ITGAL) were identified as risk genes. The gene signature generated by these genes demonstrated high accuracy in predicting psoriasis and AAA. Using five algorithms for immune infiltration analysis, an abundance of inflammatory cells was observed in high-risk subgroups. The above six genes were found to be highly expressed in both psoriasis tissue and abdominal aortic aneurysm tissue.
Conclusions : The study resulted in the identification of a novel gene signature, including six high-risk genes, that has enhanced our knowledge of the common causes and control mechanisms of psoriasis and AAA. These findings are anticipated to pave the way for promising therapeutic targets in mitigating the comorbidities of cardiovascular disease.
Keywords: abdominal aortic aneurysm; nomogram; psoriasis; signature.
© 2025 Lyu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures







Similar articles
-
A nomoscore of four genes for predicting the rupture risk in abdominal aortic aneurysm patients with osteoarthritis.Gene. 2024 Dec 30;931:148877. doi: 10.1016/j.gene.2024.148877. Epub 2024 Aug 22. Gene. 2024. PMID: 39173977
-
Interleukin 2 receptor subunit beta as a novel hub gene plays a potential role in the immune microenvironment of abdominal aortic aneurysms.Gene. 2022 Jun 15;827:146472. doi: 10.1016/j.gene.2022.146472. Epub 2022 Apr 4. Gene. 2022. PMID: 35381314
-
Comprehensive transcriptomic analysis unveils macrophage-associated genes for establishing an abdominal aortic aneurysm diagnostic model and molecular therapeutic framework.Eur J Med Res. 2024 Jun 12;29(1):323. doi: 10.1186/s40001-024-01900-w. Eur J Med Res. 2024. PMID: 38867262 Free PMC article.
-
Identification of biomarkers for abdominal aortic aneurysm in Behçet's disease via mendelian randomization and integrated bioinformatics analyses.J Cell Mol Med. 2024 May;28(10):e18398. doi: 10.1111/jcmm.18398. J Cell Mol Med. 2024. PMID: 38785203 Free PMC article.
-
FOS gene associated immune infiltration signature in perivascular adipose tissues of abdominal aortic aneurysm.Gene. 2022 Jul 15;831:146576. doi: 10.1016/j.gene.2022.146576. Epub 2022 May 11. Gene. 2022. PMID: 35568340
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
