

Effect of hydrocortisone on mortality in patients with severe community-acquired pneumonia : The REMAP-CAP Corticosteroid Domain Randomized Clinical Trial
- PMID: 40261382
- PMCID: PMC12055926
- DOI: 10.1007/s00134-025-07861-w
Effect of hydrocortisone on mortality in patients with severe community-acquired pneumonia : The REMAP-CAP Corticosteroid Domain Randomized Clinical Trial
Erratum in
-
Publisher Correction: Effect of hydrocortisone on mortality in patients with severe community-acquired pneumonia.Intensive Care Med. 2025 Jul;51(7):1415. doi: 10.1007/s00134-025-07954-6. Intensive Care Med. 2025. PMID: 40522483 Free PMC article. No abstract available.
Abstract
Purpose: To determine whether hydrocortisone improves mortality in severe community-acquired pneumonia (CAP).
Methods: In an international adaptive randomized controlled platform trial testing multiple interventions, adults admitted to the intensive care unit (ICU) with severe CAP were randomized to a 7-day course of intravenous hydrocortisone (50 mg every 6 h) or control (no corticosteroid). The primary end point was 90-day all-cause mortality, analyzed iteratively by a Bayesian hierarchical model estimating distinct treatment effects for patients presenting with influenza (Y/N) and shock (Y/N).
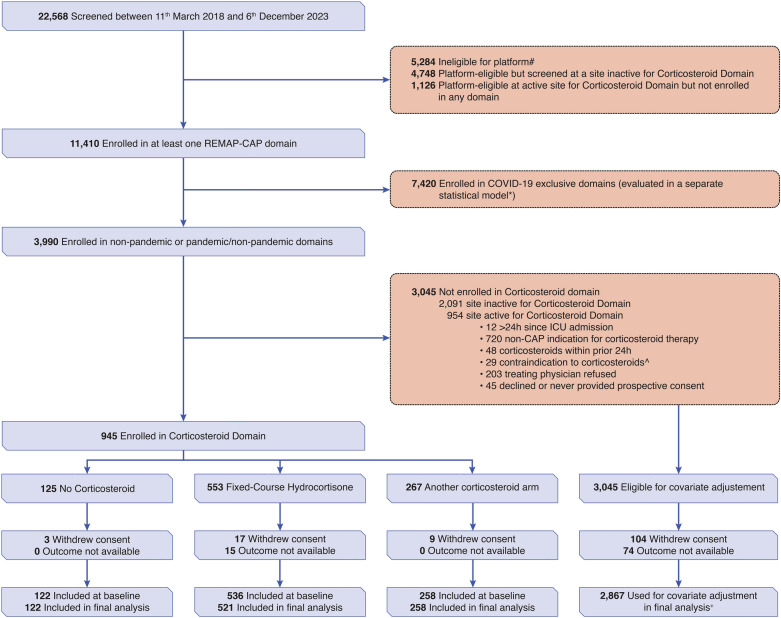
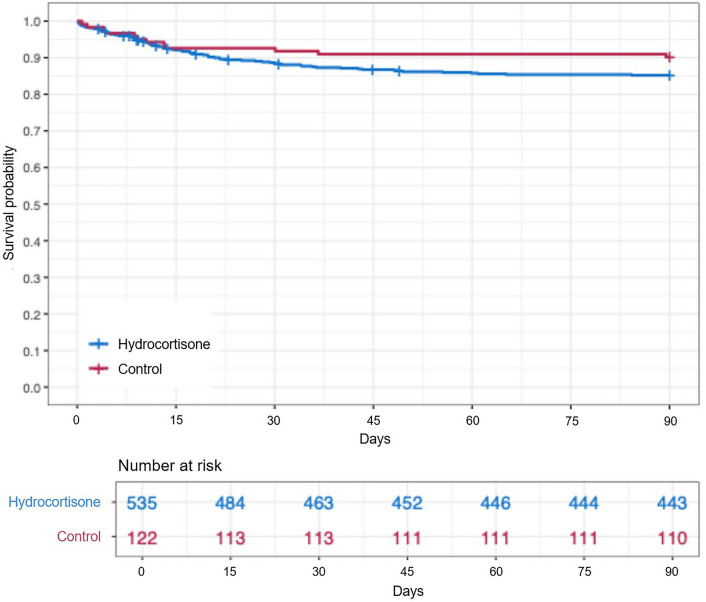
Results: Fixed 7-day course hydrocortisone enrollment was stopped for futility (< 5% probability of > 20% relative improvement). Of 658 patients enrolled, 536 were randomized to hydrocortisone and 122 to control. Vital status at day 90 was missing for 15 patients. Day 90 mortality was 15% (78/521) and 9.8% (12/122) for the hydrocortisone and control groups. The adjusted odds ratio ranged from 1.52 to 1.63 (with all 95% CrI crossing 1), while the probability of > 20% relative reduction of day 90 mortality ranged from 7.1 to 3.3% across influenza and shock strata. Results were consistent in sensitivity and pre-specified secondary outcomes. In exploratory analyses, the duration of shock appeared lower in the hydrocortisone group compared with control (median (IQR) of 2 (2-5) days compared to control 3 (2-6.75) days, p value = 0.05).
Conclusions: Among patients with severe CAP, treatment with a 7-day course of hydrocortisone, compared with no hydrocortisone, appears unlikely to yield a large reduction in mortality. Smaller benefits and possible harm are not excluded.
Trial registration: Clinicaltrials.gov identifier: NCT02735707 (registration date: November 4th, 2016).
Keywords: Adaptive platform trial; Corticosteroid; Hydrocortisone; Intensive care; Pneumonia; Shock.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: See submitted ICMJE forms for declared potential conflict of interests. Ethical approval: All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committees and with the 1964 Helsinki Declaration and its later amendments. Consent to participate: Informed consent was obtained before randomization from all patients or their surrogates, or in a deferred fashion, in accordance with local legislation.
Figures
References
-
- Sterne JAC, Murthy S, The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group et al (2020) Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA. 324:1330. 10.1001/jama.2020.17023 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- PHRC 20 0147/UPMC Learning While Doing Program, The Breast Cancer Research Foundation- Recipient: Derek C. Angus
- NUHSRO/2021/002/RO5+6/adhoc/02/LOA/National University Health System-Recipient: Matthew E. Cove
- 965313/ECRAID-Base- Recipient: Marc Bonten
- 16/631/New Zealand Health Research Council- Recipient:Colin J. McArthur
- 158584/Canadian Institute of Health Research Strategy for Patient-Oriented Research Innovative Clinical Trials Program Grant- Recipient: John C. Marshall
- NMRC/oflcg19May-0034/National Research Foundation Singapore under its Open Fund-Large Collaborative Grant-Recipient: Matthew E. Cove
- APP1101719/Australian National Health and Medical Research Council- Recipient: Steven A. Webb
- R35 GM119519/GM/NIGMS NIH HHS/United States
- PHRC 20-0147/French Ministry of Health- Recipient: Djillali Annane
- 602525/FP7 Health 2013 Innovation 1- Recipient: Marc Bonten
- CTN 2014-012/Health Research Board of Ireland-Recipient: Alistair D. Nichol
- 101003589/RECoVER- Recipient: Marc Bonten
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
