

Factors associated with local failure after stereotactic radiation to the surgical bed of patients with a single breast cancer metastasis
- PMID: 40261501
- PMCID: PMC12014713
- DOI: 10.1007/s00701-025-06520-9
Factors associated with local failure after stereotactic radiation to the surgical bed of patients with a single breast cancer metastasis
Abstract
Introduction: Breast cancer brain metastases (BCBM) are increasingly common due to improved systemic therapies prolonging survival. This study evaluates local control and factors influencing outcomes in patients with resected BCBM treated with postoperative stereotactic radiotherapy (SRT).
Methods: A retrospective review included single resected BCBM treated with postoperative SRT from 2010 to 2022. The median follow-up was 28 months (range, 14-43). Variables analyzed included tumor size, biology, surgical corridor inclusion, radiation dose, and timing of SRT. Multivariable analysis was conducted using Cox regression.
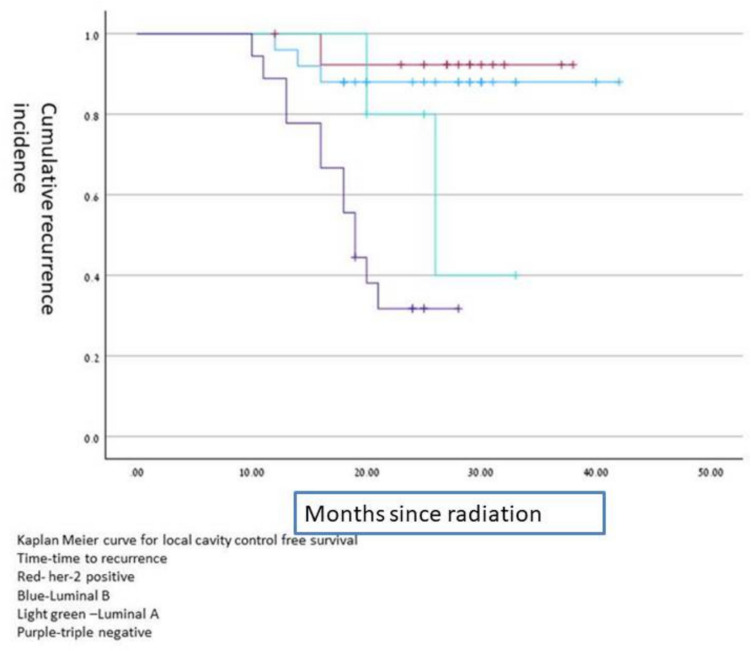
Results: 62 patients were analyzed in multivariable analysis, HER2-positive status was associated with improved local control (HR: 0.76, 95% CI: 0.36-0.88, p = 0.032), as was a higher biologically effective dose (BED > 40 Gy, HR: 0.65, 95% CI: 0.45-0.89, p = 0.028). In contrast, tumor size > 5 cm (HR: 2.1, 95% CI: 1.7-4.6, p = 0.021) and delayed initiation of SRT beyond 28 days post-surgery (HR: 2.7, 95% CI: 1.9-4.7, p = 0.015) were associated with worse outcomes. Age, cystic metastases, inclusion of surgical corridor, and tumor location were not significantly related to local control. Radiation necrosis occurred in 13% of patients, predominantly asymptomatic.
Conclusion: Postoperative SRT provides effective local control in resected BCBM. In multivariable analysis, HER2 positivity, higher BED, and timely SRT significantly influenced outcomes, while larger tumor size and delayed treatment were negative prognostic factors. Future research should optimize dosimetric strategies and integrate systemic therapy to improve local and intracranial control.
Keywords: Brain metastases; Breast cancer; Craniotomy; Postoperative radiotherapy; Radiosurgery.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: IRB approval number 0265–23-SMC. Consent for publication: This article has not been published before. All authors read this manuscript and approved it submission. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bartsch R, Berghoff AS, Preusser M (2014) Breast cancer brain metastases responding to primary systemic therapy with t-dm1. J Neurooncol 116:205–206 - PubMed
-
- Bartsch R, Berghoff AS, Vogl U et al (2015) Activity of t-dm1 in her2-positive breast cancer brain metastases. Clin Exp Metastasis 32:729–737 - PubMed
-
- Brown P, Asher A, Ballman K, Farace E, Cerhan J, Anderson SK, Carrero X, Barker F II, Deming R, Burri S, Ménard C, Chung C, Stieber V, Pollock B, Galanis E, Buckner J, Jaeckle K (2015) BMET-05: NCCTG N0574 (ALLIANCE): a phase III randomized trial of whole brain radiation therapy (WBRT) in addition to radiosurgery (SRS) in patients with 1 to 3 brain metastases. Neuro Oncol 17(Suppl 5):v45–46. 10.1093/neuonc/nov208.05
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
