

Stewart's theory and acid-base changes induced by crystalloid infusion in humans: a randomized physiological trial
- PMID: 40263186
- PMCID: PMC12014888
- DOI: 10.1186/s13613-025-01473-9
Stewart's theory and acid-base changes induced by crystalloid infusion in humans: a randomized physiological trial
Abstract
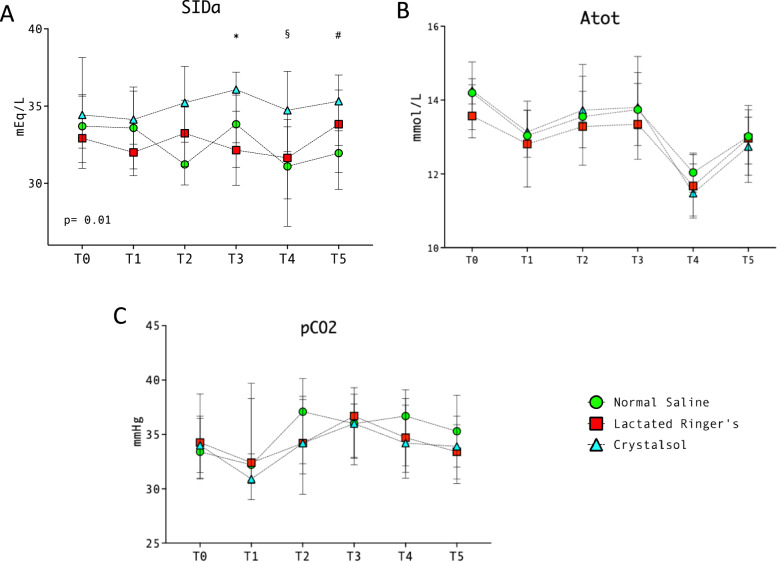
Background: Stewart's acid-base theory states that, under isocapnic conditions, crystalloid infusion affects plasma pH due to changes in strong ion difference and total weak acid concentration: a comprehensive study also assessing renal response and hemodilution effects has not been conducted in humans. We aimed to evaluate Stewart's approach during crystalloid infusion in humans.
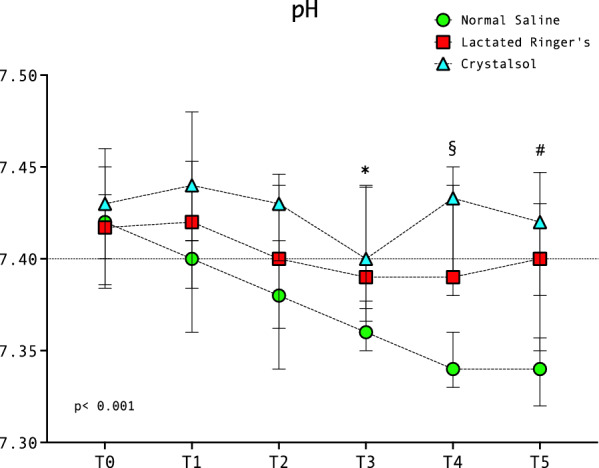
Methods: In this randomized trial, patients undergoing surgery with minimal blood losses were randomized to receive to normal saline (chloride content 154 mEq/L, strong ion difference 0 mEq/L), lactated Ringer's (chloride content 112 mEq/L, strong ion difference 29 mEq/L) or Crystalsol (chloride content 98 mEq/L, strong ion difference 50 mEq/L): patients received 10 ml/kg immediately after intubation, and 20 ml/kg after 2 h. Plasma/urinary acid-base and electrolytes were measured before study start and then at prespecified timepoints. The primary endpoint was pH one hour after the second fluid bolus: secondary outcomes included urinary/plasmatic electrolyte concentrations and strong ion difference during the study.
Results: Forty-five patients were enrolled (15 in each group). The extent of hemodilution achieved with the first (median [Interquartile range]: saline 9% [6-15], Ringer's 7% [4-9], Crystalsol 8% [5-12]) and the second fluid bolus (saline 13% [5-17], Ringer's 12% [9-15], Crystalsol 15% [10-20]) was not different between groups (p = 0.39 and p = 0.19, respectively). Patients in saline group received more chloride (449 mEq [383-495]) vs. Ringer's (358 mEq [297-419]) and Crystalsol groups (318 mEq [240-366]) (p = 0.001). One hour after the second bolus, pH was lower in saline group (7.34 [7.32-7.36]) vs. Ringer's (7.40 [7.35-7.43) and Crystalsol groups (7.42 [7.38-7.44]) (both p < 0.01), since plasma chloride increased significantly over time in saline group but not in Ringer's and Crystalsol groups. Overall chloride urinary excretion was not different between study groups (saline 36 mEq [28-64], Ringer's 42 mEq [29-68], Crystalsol 44 mEq [27-56], p = 0.60) but, at the end of experiments, urinary chloride concentration was higher and diuresis was lower in saline group vs. Ringer's and Crystalsol groups (p = 0.01, p = 0.04, respectively).
Conclusions: Consistent with Stewart's approach, crystalloid solutions with high chloride content lower pH due to reduced strong ion difference, progressive hemodilutional acidosis and limited renal response to chloride load.
Trial registration: Registered on clinicaltrials.gov (NCT03507062) on April, 24th 2018.
Keywords: Acid–base balance; Chloride; Crystalloids; Stewart; Strong ion difference.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by local Ethics Committee and informed consent was obtained by enrolled patients according to committee recommendations. Consent for publication: Not applicable. Competing interests: The authors declare that they have no conflicts of interests for the material discussed in the manuscript.
Figures




References
-
- Glassford NJ, Bellomo R. The complexities of intravenous fluid research: questions of scale, volume, and accumulation. Korean J Crit Care Med. 2016;31:276–99. - DOI
-
- Messina A, Robba C, Calabrò L, Zambelli D, Iannuzzi F, Molinari E, et al. Association between perioperative fluid administration and postoperative outcomes: a 20-year systematic review and a meta-analysis of randomized goal-directed trials in major visceral/noncardiac surgery. Crit Care. 2021;25:43. - DOI - PMC - PubMed
-
- Van Regenmortel N, Verbrugghe W, Roelant E, Van den Wyngaert T, Jorens PG. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intensive Care Med. 2018;44:409–17. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
