

Nomogram model for the preoperative prediction of spread through air spaces in sub-centimeter non-small cell lung cancer
- PMID: 40264135
- PMCID: PMC12016363
- DOI: 10.1186/s13019-025-03441-7
Nomogram model for the preoperative prediction of spread through air spaces in sub-centimeter non-small cell lung cancer
Abstract
Introduction: To construct and validate a nomogram risk prediction model based on clinical characteristics and radiological features to predict spread through air spaces (STAS) of stage IA sub-centimeter non-small cell lung cancer.
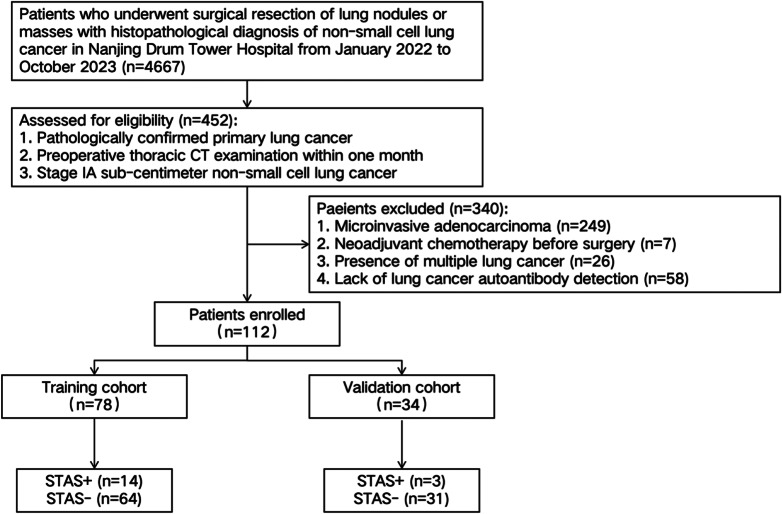
Methods: 112 patients who underwent surgical treatment in Nanjing Drum Tower Hospital with pathologically diagnosed stage IA sub-centimeter non-small cell lung cancer were retrospectively collected. The training cohort and the validation cohort were chosen in a 7:3 ratio. Based on the presence or absence of STAS in pathology results, they were divided into STAS positive and STAS negative groups. The independent risk predictors of STAS in clinical characteristics and radiological features were selected by univariate and multivariate logistic regression analysis and then used to construct a nomogram. The sensitivity and specificity were calculated based on the Youden index, area under the curve (AUC), calibration curves and decision curve analysis (DCA) were used to evaluate the performance of the model.
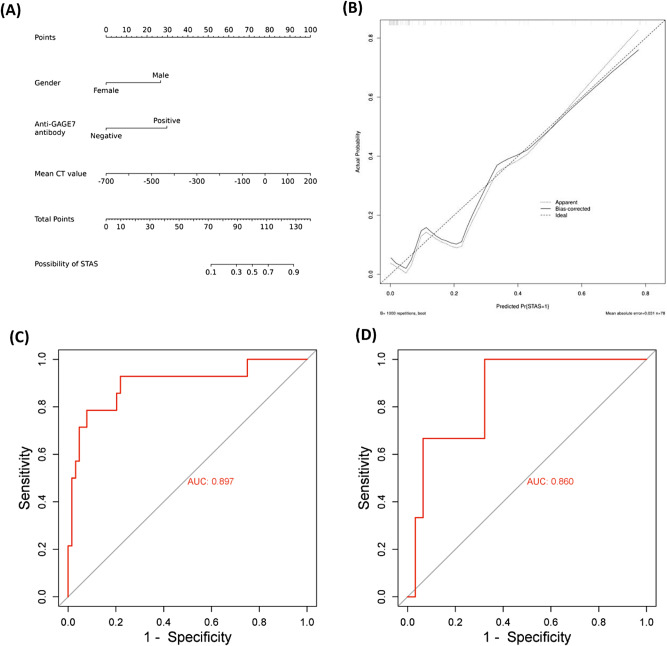
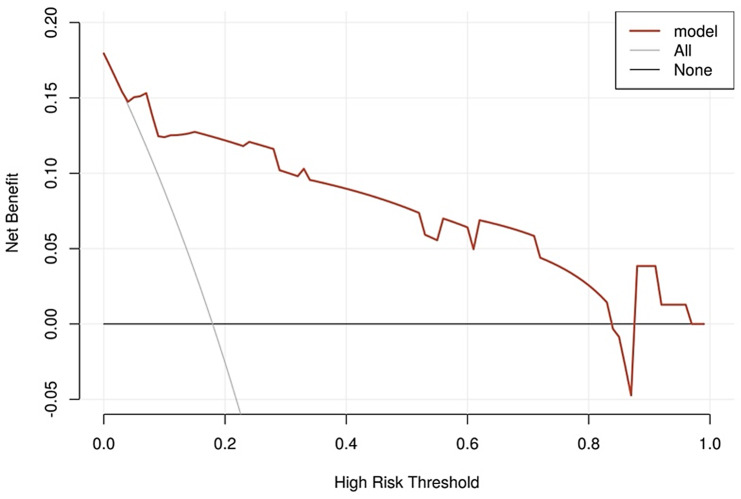
Results: The incidence of STAS in the training cohort was 17.9%. Univariate logistic regression analysis showed that male, anti-GAGE7 antibody positive and mean CT value were associated with the occurrence of STAS; multivariate logistic regression analysis showed that male (OR = 7.900, 95%CI: 1.502-41.545), anti-GAGE7 antibody positive (OR = 10.065, 95%CI: 1.256-80.659) and mean CT value (OR = 1.009, 95%CI: 1.004-1.014) were independent predictors for STAS. The nomogram based on the above factors achieved good predictive performance for STAS with AUC was 0.897 (sensitivity was 0.929, specificity was 0.781) in the training cohort and 0.860 in the validation cohort. The calibration curve and DCA validated the good performance of the model.
Conclusion: The nomogram model established in this study had good predictive performance for STAS status of sub-centimeter lung cancer, and provide reference significance for preoperative planning of patients.
Keywords: Nomogram; Prediction model; Spread through air spaces; Sub-centimeter lung cancer.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: This retrospective study was approved by the Institutional Ethics Committee of Nanjing Drum Tower Hospital. Written informed consent was waived due to the retrospective nature of this study. Conflict of interest: The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Nomogram based on clinical characteristics and radiological features for the preoperative prediction of spread through air spaces in patients with clinical stage IA non-small cell lung cancer: a multicenter study.Diagn Interv Radiol. 2023 Nov 7;29(6):771-785. doi: 10.4274/dir.2023.232404. Epub 2023 Sep 19. Diagn Interv Radiol. 2023. PMID: 37724737 Free PMC article. Clinical Trial.
-
A nomogram integrating the clinical and CT imaging characteristics for assessing spread through air spaces in clinical stage IA lung adenocarcinoma.Front Immunol. 2025 Apr 11;16:1519766. doi: 10.3389/fimmu.2025.1519766. eCollection 2025. Front Immunol. 2025. PMID: 40292286 Free PMC article.
-
Preoperative nomogram for predicting spread through air spaces in clinical-stage IA non-small cell lung cancer using 18F-fluorodeoxyglucose positron emission tomography/computed tomography.J Cancer Res Clin Oncol. 2024 Apr 10;150(4):185. doi: 10.1007/s00432-024-05674-w. J Cancer Res Clin Oncol. 2024. PMID: 38598007 Free PMC article.
-
Diagnostic performance of radiomics analysis for pulmonary cancer airway spread: a systematic review and meta-analysis.Diagn Interv Radiol. 2025 Apr 28;31(3):215-225. doi: 10.4274/dir.2024.242852. Epub 2025 Apr 7. Diagn Interv Radiol. 2025. PMID: 40192338 Free PMC article.
-
A narrative review of preoperative CT for predicting spread through air spaces of lung cancer.Transl Lung Cancer Res. 2025 Apr 30;14(4):1471-1481. doi: 10.21037/tlcr-24-952. Epub 2025 Apr 27. Transl Lung Cancer Res. 2025. PMID: 40386727 Free PMC article. Review.
References
-
- Siegel R L, Giaquinto A N Jemala. Cancer statistics, 2024 [J]. CA Cancer J Clin. 2024;74(1):12–49. - PubMed
-
- Suzuki K, Watanabe S I, Wakabayashi M, et al. A single-arm study of sublobar resection for ground-glass opacity dominant peripheral lung cancer [J]. J Thorac Cardiovasc Surg. 2022;163(1):289–e3012. - PubMed
-
- Saji H, Okada M, Tsuboi M, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial [J]. Lancet. 2022;399(10335):1607–17. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
