

Using panoramic radiographs to assess the probability of causing oroantral communication following tooth removal. A retrospective cross-sectional study
- PMID: 40266377
- PMCID: PMC12018612
- DOI: 10.1007/s00784-025-06335-z
Using panoramic radiographs to assess the probability of causing oroantral communication following tooth removal. A retrospective cross-sectional study
Abstract
Objectives: To preoperatively assess the probability of oroantral communication (OAC) following the removal of maxillary (pre)molars using panoramic radiographs (PAN) and to assess the OAC-rate.
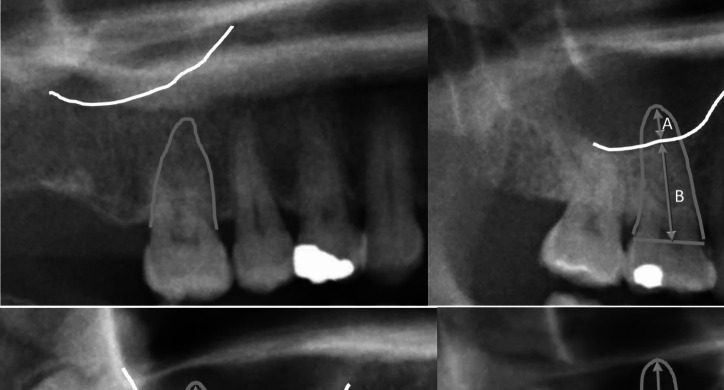
Materials and methods: During a 4,5-year period, patient characteristics of removals of maxillary (pre-)molars were recorded: 'sex', age, 'sidedness', 'type of tooth', 'reason for removal'' and 'occurrence of OAC'. On the PAN of OAC-cases and of 100 control cases, the 'Fraction of the Root Overlapping the Maxillary Sinus' (FROMS) was calculated. The OAC-rate was reported overall, per tooth type and for four diagnostic classes: A: no overlap, B: 0.1-25%, C: 25.1-50% and D > 50% overlap. Univariate tests and regression analysis were performed to test the association between OAC-rate and 'FROMS', 'sex', age, 'sidedness', 'type of tooth', 'reason for removal'.
Results: Of 2340 maxillary (pre-)molars removed, 112 resulted in OAC (OAC-rate of 4.8% (95%CI 3.9%-5.7%)) The FROMS diagnostic class was significantly associated with the OAC-rate (χ2 = 42.90 df3, p < 0.0001). For the four diagnostic classes the risk of OAC was (A) 1.0%, (B) 3.3%. (C) 10.1% and (D) 17.7%. The first molar showed highest OAC-rate with 7.0%. No association between OAC-rate and 'sex', age, 'sidedness', 'type of tooth', 'reason for removal' was found.
Conclusions: FROMS is a valid indicator of OAC probability. The overall OAC-rate was 4.8% and was highest in first molar removal.
Clinical relevance: Dentists and oral surgeons using PAN to assess OAC probability, can anticipate possible OAC and counsel patients.
Keywords: Adverse Effects; Oroantral Fistula; Panoramic Radiography; Peroperative Complications; Tooth Extraction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. This study was granted the approval of the Board of Directors of the Diakonessenhuis following the recommendation of its Research Bureau (Appendix 1). The approval of the Ethical Review Board of the Academic Center for Dentistry Amsterdam (ACTA) was also obtained, under number 2022–35410. The study was ruled not to be subject to the Medical Research Involving Human Subjects Act (WMO) (Appendix 2). Informed consent: No Informed consent was applicable for this study. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Evaluation of clinical and radiographic warning signs for prediction of oroantral communication following tooth extractions.Clin Oral Investig. 2024 Oct 23;28(11):609. doi: 10.1007/s00784-024-06000-x. Clin Oral Investig. 2024. PMID: 39443353 Free PMC article.
-
Risk factors associated with oroantral perforation during surgical removal of maxillary third molar teeth.Oral Maxillofac Surg. 2016 Dec;20(4):369-375. doi: 10.1007/s10006-016-0574-1. Epub 2016 Sep 13. Oral Maxillofac Surg. 2016. PMID: 27624331
-
Risk factor analysis for perioperative complications in impacted third molar surgery - a single center experience.Oral Maxillofac Surg. 2024 Sep;28(3):1127-1138. doi: 10.1007/s10006-024-01232-3. Epub 2024 Mar 1. Oral Maxillofac Surg. 2024. PMID: 38427098
-
Risk factors in oroantral communication while extracting the upper third molar: Systematic review.Dent Med Probl. 2018 Jan-Mar;55(1):69-74. doi: 10.17219/dmp/80944. Dent Med Probl. 2018. PMID: 30152638
-
Implant Placement after Closure of Oroantral Communication by Sinus Bone Graft Using a Collagen Barrier Membrane in the Shape of a Pouch: A Case Report and Review of the Literature.Medicina (Kaunas). 2021 Jun 16;57(6):626. doi: 10.3390/medicina57060626. Medicina (Kaunas). 2021. PMID: 34208644 Free PMC article. Review.
References
-
- Iwanaga J, Wilson C, Lachkar S, Tomaszewski KA, Walocha JA, Tubbs RS (2019) Clinical anatomy of the maxillary sinus: Application to sinus floor augmentation. Anat Cell Biol 52:17–24. https://doi-org.vu-nl.idm.oclc.org/10.5115/acb.2019.52.1.17 - DOI - PMC - PubMed
-
- Baart JA, Bretschneider JH, de Visscher JG, van der Waal I (2012) Afwijkingen van de sinus maxillaris: een overzicht. Ned Tijdschr Tandheelkd 119:199–204 - PubMed
-
- Dym H, Wolf JC (2012) Oroantral communication. Oral Maxillofac Surg Clin North Am 24:239–247. https://doi-org.vu-nl.idm.oclc.org/10.1016/j.coms.2012.02.005 - DOI - PubMed
-
- Malik N (2012) Textbook of Oral and Maxillofacial Surgery. JP Medical Ltd, London
-
- Simuntis R, Kubilius R, Vaitkus S (2014) Odontogenic maxillary sinusitis: a review. Stomatologija 16:39–43 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
