

Geographic and age variations in mutational processes in colorectal cancer
- PMID: 40267983
- PMCID: PMC12221974
- DOI: 10.1038/s41586-025-09025-8
Geographic and age variations in mutational processes in colorectal cancer
Abstract
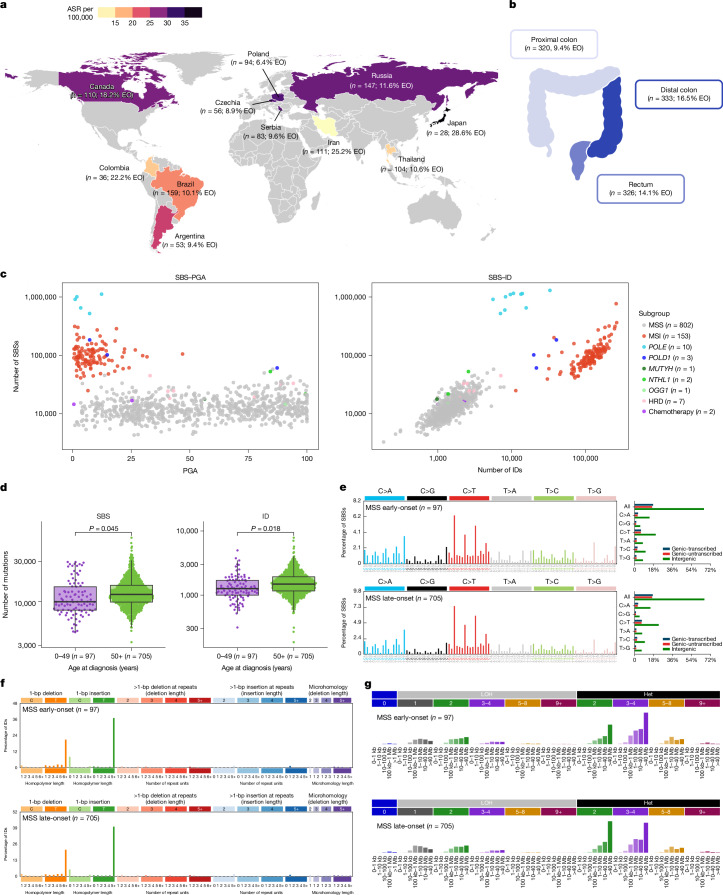
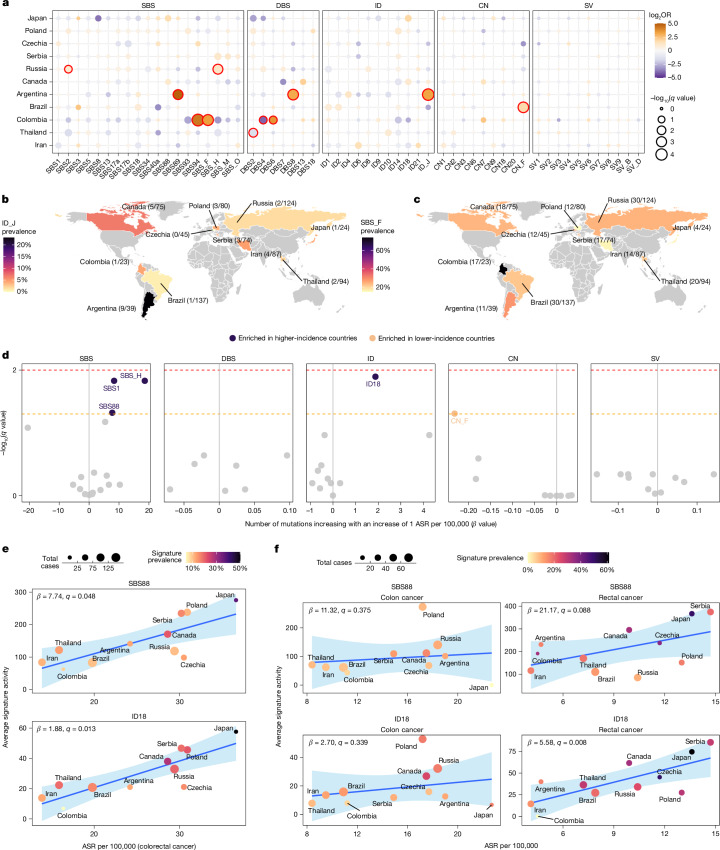
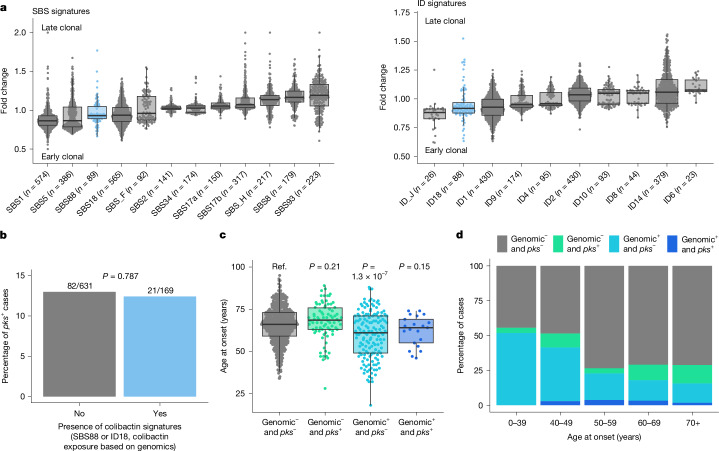
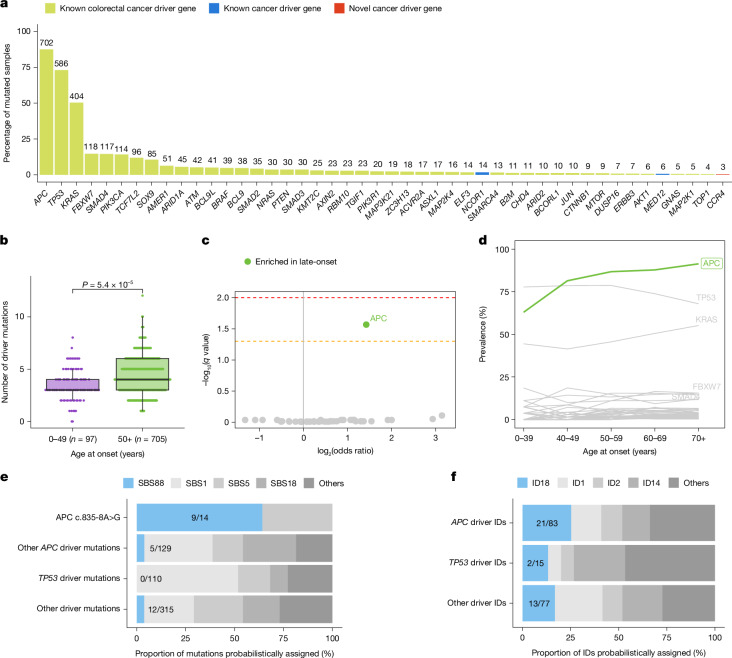
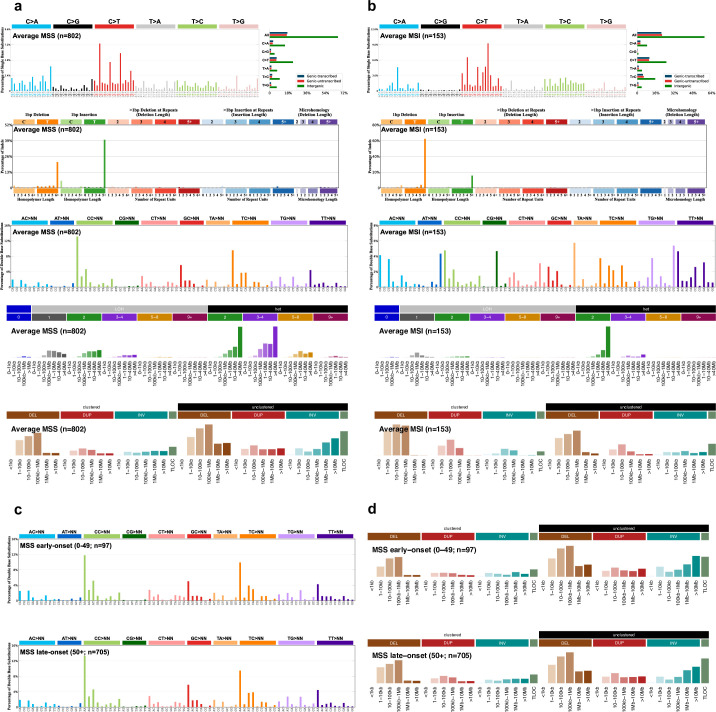
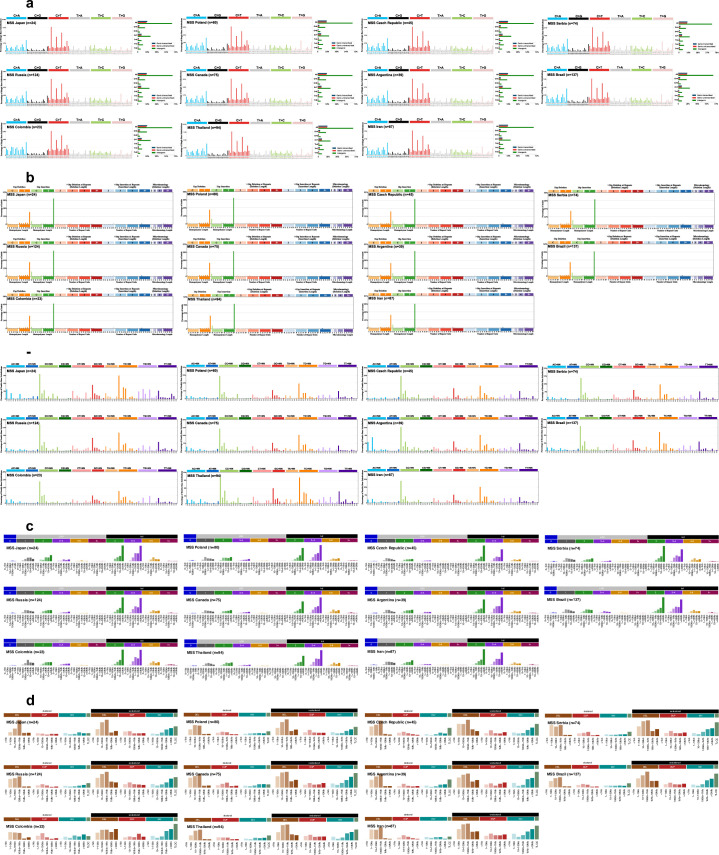
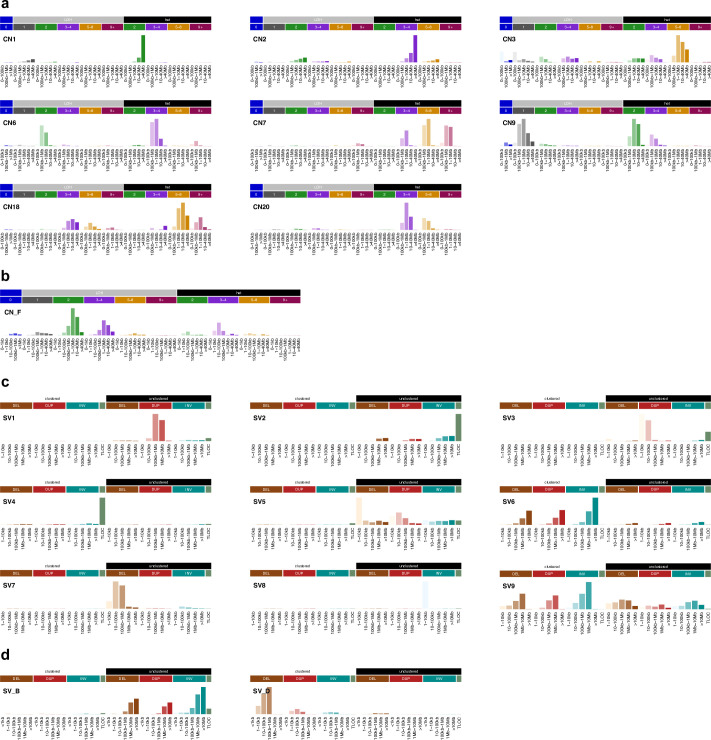
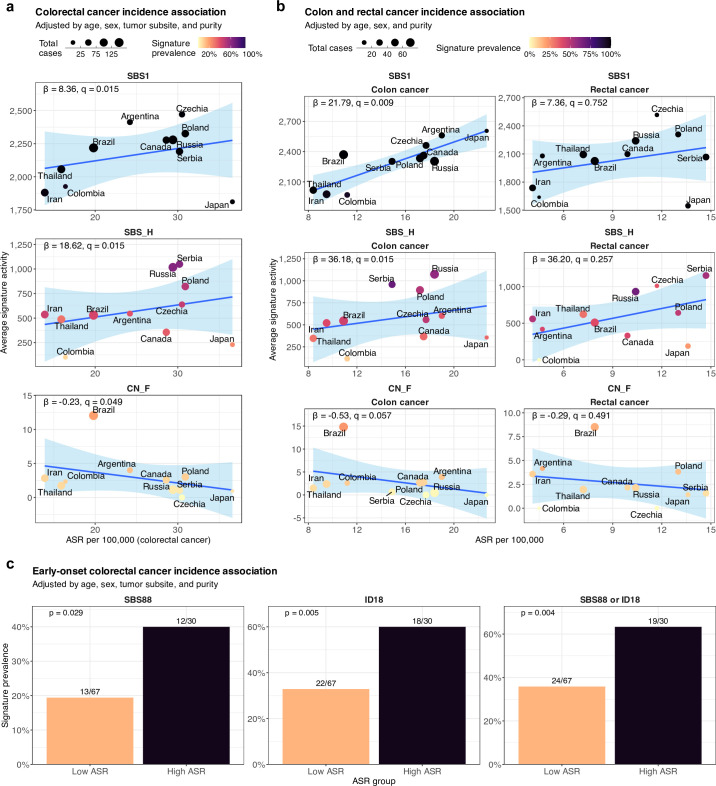
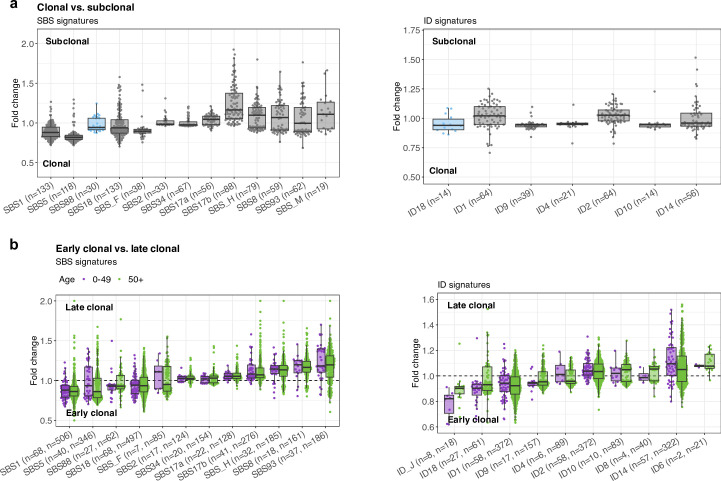
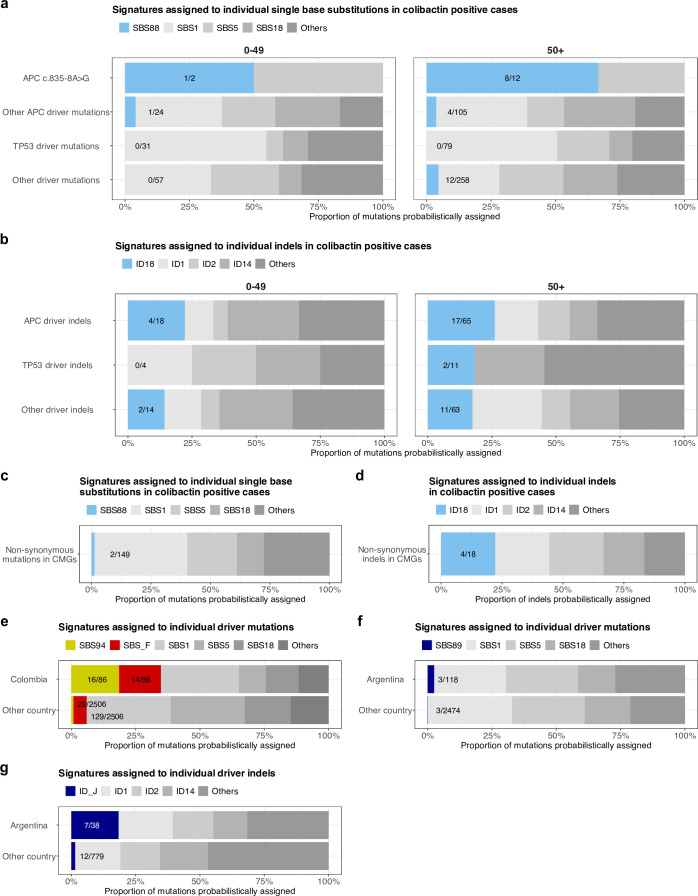
Incidence rates of colorectal cancer vary geographically and have changed over time1. Notably, in the past two decades, the incidence of early-onset colorectal cancer, which affects individuals below 50 years of age, has doubled in many countries2-5. The reasons for this increase are unknown. Here we investigate whether mutational processes contribute to geographic and age-related differences by examining 981 colorectal cancer genomes from 11 countries. No major differences were found in microsatellite-unstable cancers, but variations in mutation burden and signatures were observed in the 802 microsatellite-stable cases. Multiple signatures, most with unknown aetiologies, exhibited varying prevalence in Argentina, Brazil, Colombia, Russia and Thailand, indicating geographically diverse levels of mutagenic exposure. Signatures SBS88 and ID18, caused by the bacteria-produced mutagen colibactin6,7, had higher mutation loads in countries with higher colorectal cancer incidence rates. SBS88 and ID18 were also enriched in early-onset colorectal cancers, being 3.3 times more common in individuals who were diagnosed before 40 years of age than in those over 70 years of age, and were imprinted early during colorectal cancer development. Colibactin exposure was further linked to APC driver mutations, with ID18 being responsible for about 25% of APC driver indels in colibactin-positive cases. This study reveals geographic and age-related variations in colorectal cancer mutational processes, and suggests that mutagenic exposure to colibactin-producing bacteria in early life may contribute to the increasing incidence of early-onset colorectal cancer.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: L.B.A. is a co-founder, chief scientific officer, scientific advisory member and consultant for, has equity in and receives income from io9. The terms of this arrangement have been reviewed and approved by the University of California, San Diego in accordance with its conflict of interest policies. L.B.A. is also a compensated member of the scientific advisory board of Inocras. L.B.A.’s spouse is an employee of Hologic, Inc. E.N.B. is a consultant for, has equity in, and receives income from io9. A.A. and L.B.A. declare US provisional patent application filed with UCSD with serial number 63/366,392. E.N.B. and L.B.A. declare US provisional patent application filed with UCSD with serial number 63/269,033. L.B.A. also declares US provisional applications filed with UCSD with serial numbers 63/289,601 and 63/412,835, as well as international patent application PCT/US2023/010679. L.B.A. is also an inventor on US Patent 10,776,718 for source identification by non-negative matrix factorization. M.R.S. is founder, consultant, and stockholder for Quotient Therapeutics. L.B.A., M.D.-G., P.B., S.P., M.R.S. and S. Moody declare a European patent application with application number EP25305077.7. T.D.L. is a co-founder and CSO of Microbiotica. All other authors declare no competing interests.
Figures





Update of
-
Geographic and age-related variations in mutational processes in colorectal cancer.medRxiv [Preprint]. 2025 Feb 21:2025.02.13.25322219. doi: 10.1101/2025.02.13.25322219. medRxiv. 2025. Update in: Nature. 2025 Jul;643(8070):230-240. doi: 10.1038/s41586-025-09025-8. PMID: 40034755 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
