

Enhancing long-term adherence in elderly stroke rehabilitation through a digital health approach based on multimodal feedback and personalized intervention
- PMID: 40268986
- PMCID: PMC12019390
- DOI: 10.1038/s41598-025-95726-z
Enhancing long-term adherence in elderly stroke rehabilitation through a digital health approach based on multimodal feedback and personalized intervention
Abstract
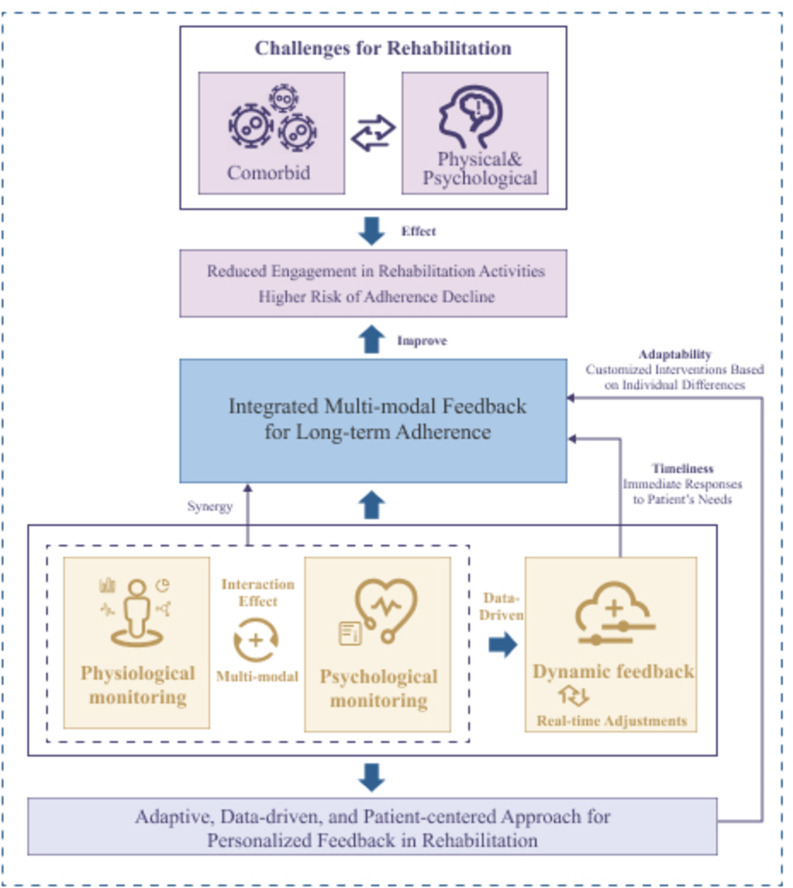
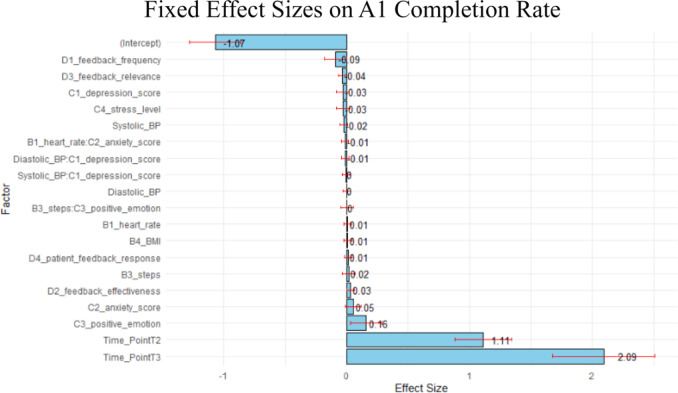
Multimodal digital health technologies aim to improve long-term adherence in stroke patients through personalized feedback and psychological monitoring. However, the interactive effects of physiological and psychological factors on rehabilitation adherence remain unclear. This study evaluates personalized feedback, physiological and psychological factors, and their independent and synergistic effects to optimize rehabilitation adherence in elderly stroke patients. This study was designed as a longitudinal study, with data collected from 180 participants across two central hospitals between March and September 2024. A linear mixed effects model (LMM) was used to analyze the impact of physiological monitoring, psychological monitoring, and personalized feedback mechanisms on long-term patient adherence. Data were gathered through structured questionnaires, resulting in a final sample size of 540 data points. The time effect has a significant positive effect on rehabilitation compliance. The rehabilitation plan completion rate (A1) increases by 1.25 (t = 34.25) and 2.28 units (t = 62.56) in the mid-term follow-up (T2) and long-term follow-up (T3) respectively; the self-reported compliance score (A2) increases by 1.12 (t = 31.39) and 2.3 points (t = 64.27) at T2 and T3 respectively; the completion of specific activities (A3) increases by 1.37 (t = 50.34) and 2.34 units (t = 86.26); the number of interruptions (A4) decreases by 0.89 (t = -17.31) and 2.11 times (t = -41.17) respectively. In personalized feedback, high-quality feedback (D2) significantly promotes compliance (β = 0.0318, t = 2.08), while excessively frequent feedback (D1) showes a negative impact (β=-0.0914, t=-1.93 ). In terms of psychological factors, positive emotion (C3) has a significant positive effect on compliance (β = 0.1572, t = 2.695), while depressed emotion (C1) significantly reduces interruption behavior (β=-0.0885). The interaction effect between physiological factors and psychological factors is not significant, indicating that their influence is relatively independent. This study demonstrates that personalized feedback, psychological support, and time effects are essential for enhancing rehabilitation adherence in elderly stroke patients. High-quality, relevant feedback significantly improves adherence, while ineffective feedback may have adverse effects. Positive emotions within psychological factors promote adherence, whereas depressive emotions hinder recovery, underscoring the importance of psychological support. Although physiological and psychological factors lack significant interactive effects, their independent influences merit attention and optimization in rehabilitation interventions.
Keywords: Adherence; Elderly patients; Linear mixed effects model; Personalized feedback intervention; Rehabilitation; Stroke.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: This study was reviewed and approved by the Ethics Committee of Wuhan Union Hospital (Approval Number: WHUHTMC-K-2024306). The committee confirmed that the project aligns with the principles of the Declaration of Helsinki and medical ethics requirements, and it granted approval for the study within the specified period. Written informed consent was obtained from all participants after explaining the study’s purpose, procedures, and their rights, including the right to withdraw at any time. Data collection and analysis adhered to strict anonymization protocols to ensure participant privacy, with secure data storage in compliance with relevant regulations. Consent for publication: Consent for publication was obtained from all individual participants included in the study. Participants were informed that their anonymized data would be used for research and publication purposes, and they provided consent for their data to be shared in an academic setting without revealing their identities. Consent to participate: Informed consent was obtained from all individual participants included in the study. All participants were provided with comprehensive information regarding the study’s purpose, procedures, potential risks, and their rights, including the right to withdraw at any time without penalty. Consent forms were signed prior to participation, ensuring that each participant voluntarily agreed to take part in the study.
Figures
Similar articles
-
Implementation interventions to promote the uptake of evidence-based practices in stroke rehabilitation.Cochrane Database Syst Rev. 2020 Oct 15;10(10):CD012575. doi: 10.1002/14651858.CD012575.pub2. Cochrane Database Syst Rev. 2020. PMID: 33058172 Free PMC article.
-
Barriers to adherence of stroke rehabilitation: therapist and patient's perspective.J Pak Med Assoc. 2025 Apr;75(4):569-577. doi: 10.47391/JPMA.11551. J Pak Med Assoc. 2025. PMID: 40269364
-
Does feedback on daily activity level from a Smart watch during inpatient stroke rehabilitation increase physical activity levels? Study protocol for a randomized controlled trial.Trials. 2018 Mar 9;19(1):177. doi: 10.1186/s13063-018-2476-z. Trials. 2018. PMID: 29523170 Free PMC article.
-
Measurement of adherence to home-based exercises among community-dwelling stroke survivors in India.Physiother Res Int. 2020 Apr;25(2):e1827. doi: 10.1002/pri.1827. Epub 2019 Dec 26. Physiother Res Int. 2020. PMID: 31880059
-
Digital technology for delivering and monitoring exercise programs for people with cystic fibrosis.Cochrane Database Syst Rev. 2023 Jun 9;6(6):CD014605. doi: 10.1002/14651858.CD014605.pub2. Cochrane Database Syst Rev. 2023. PMID: 37294546 Free PMC article. Review.
References
-
- Hilkens, N. A., Casolla, B., Leung, T. W., De Leeuw, F. E. & Stroke Lancet ;403(10446):2820–2836. doi:10.1016/S0140-6736(24)00642-1 (2024). - PubMed
-
- Stinear, C. M., Lang, C. E., Zeiler, S. & Byblow, W. D. Advances and challenges in stroke rehabilitation. Lancet Neurol.19 (4), 348–360. 10.1016/S1474-4422(19)30415-6 (2020). - PubMed
-
- Murray, C. J. & Lopez, A. D. Alternative projections of mortality and disability by cause 1990–2020: global burden of disease study. Lancet349 (9064), 1498–1504. 10.1016/S0140-6736(96)07492-2 (1997). - PubMed
-
- Teasell, R. et al. Canadian stroke best practice recommendations: rehabilitation, recovery, and community participation following stroke. Part one: rehabilitation and recovery following stroke; 6th edition update 2019. Int. J. Stroke. 15 (7), 763–788. 10.1177/1747493019897843 (2020). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
