

First-in-human implementation of a bidirectional somatosensory neuroprosthetic system with wireless communication
- PMID: 40269935
- PMCID: PMC12020317
- DOI: 10.1186/s12984-025-01613-z
First-in-human implementation of a bidirectional somatosensory neuroprosthetic system with wireless communication
Abstract
Background: Limitations in upper limb prosthesis function and lack of sensory feedback are major contributors to high prosthesis abandonment rates. Peripheral nerve stimulation and intramuscular recording can restore touch and relay motor intentions for individuals with upper limb loss. Percutaneous systems have enabled significant progress in implanted neural interfaces but require chronic lead maintenance and unwieldy external equipment. Fully implanted sensorimotor systems without percutaneous leads are crucial for advancing implanted neuroprosthetic technologies to long-term community use and commercialization.
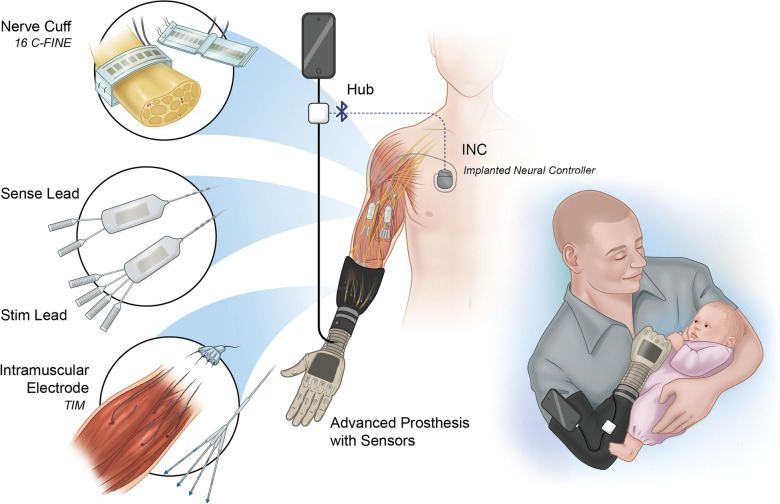
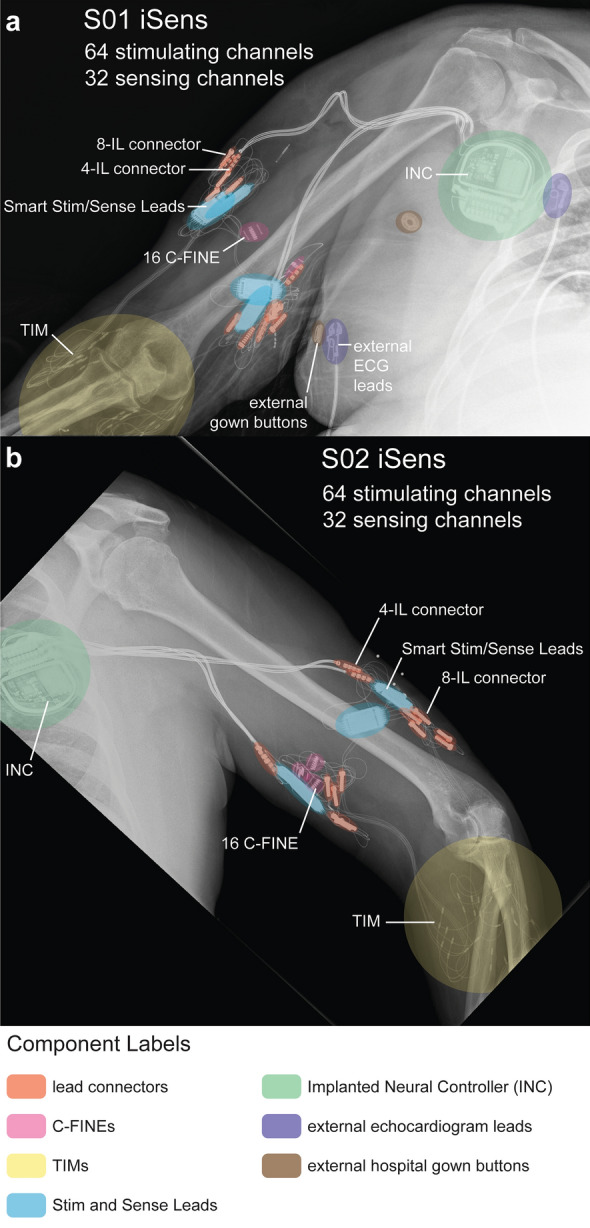
Methods: We present the first-in-human technical performance of the implanted Somatosensory Electrical Neurostimulation and Sensing (iSens®) system-an implanted, high-channel count myoelectric sensing and nerve stimulation system that uses wireless communication for advanced prosthetic systems. Two individuals with unilateral transradial amputations received iSens® with four 16-channel composite Flat Interface Nerve Electrodes (C-FINEs) and four Tetra Intramuscular (TIM) electrodes. This study achieved two key objectives to demonstrate system feasibility prior to long-term community use: (1) evaluating the chronic stability of extraneural cuff electrodes, intramuscular electrodes, and active implantable devices in a wirelessly connected system and (2) assessing the impacts of peripheral nerve stimulation on three degree-of-freedom controller performance in a wirelessly connected system to validate iSens® as a bidirectional interface.
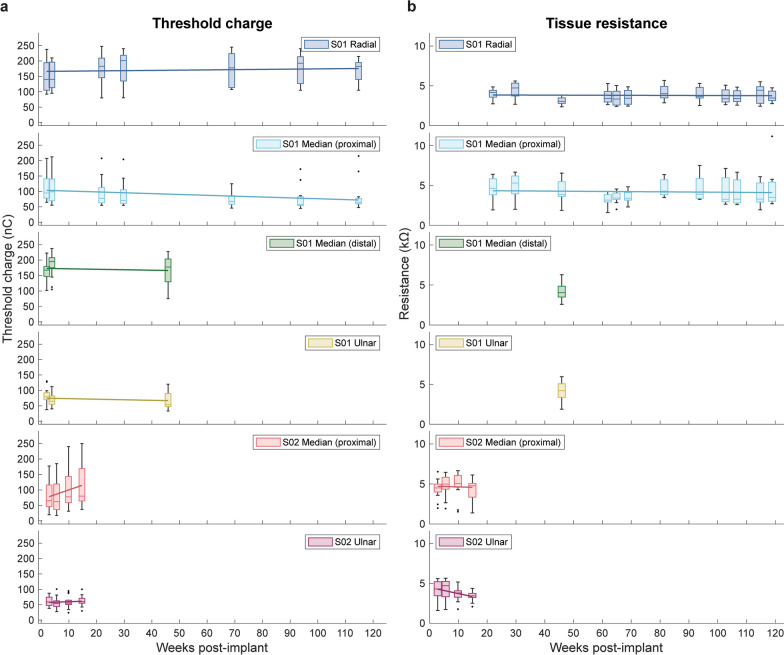
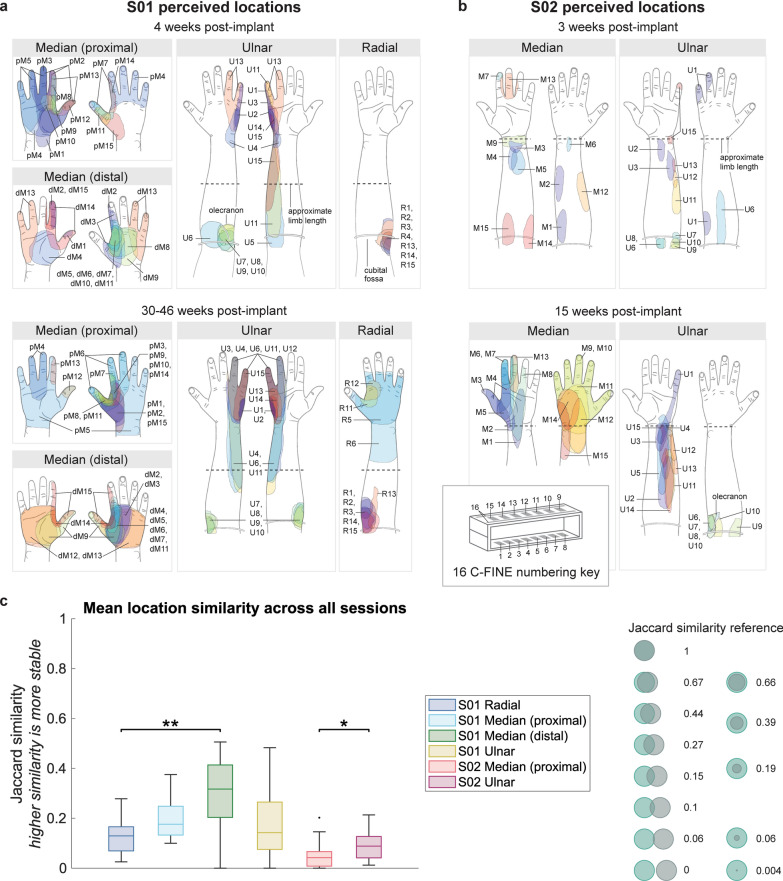
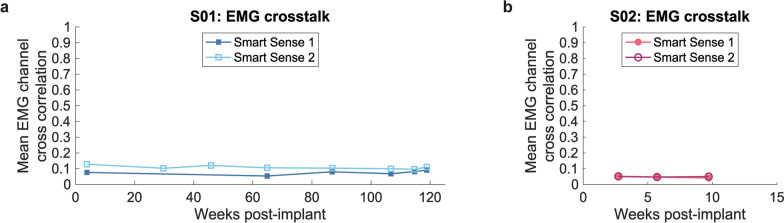
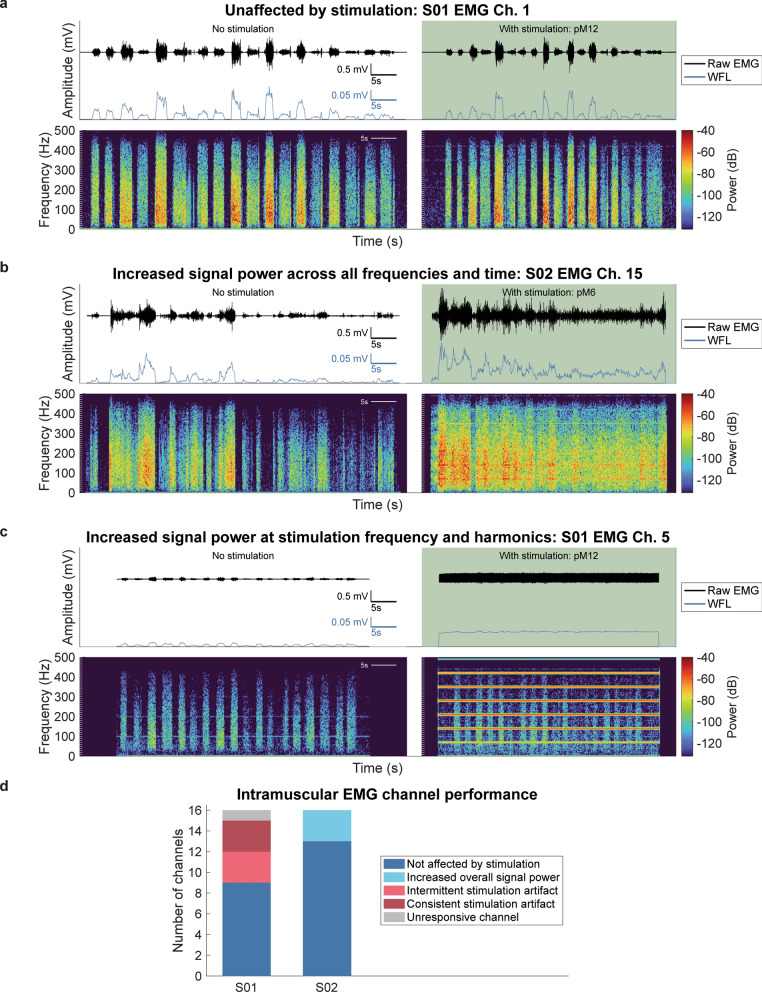
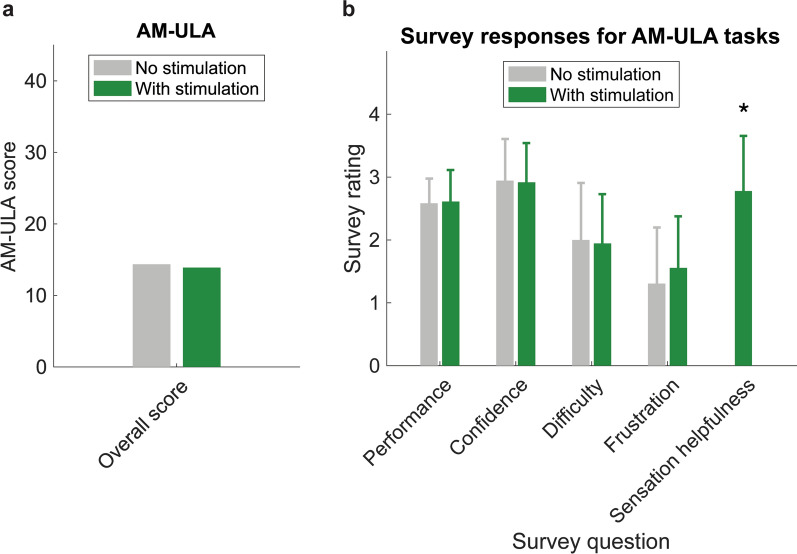
Results: Similar to prior percutaneous systems, we demonstrate chronically stable extraneural cuff electrodes and intramuscular electrodes in a wirelessly connected implanted system for more than two years in one participant and four months in the second participant, whose iSens® system was explanted due to an infection of unknown origin. Using an artificial neural network controller trained on implanted electromyographic data collected during known hand movements, one participant commanded a virtual hand and sensorized prosthesis in 3 degrees-of-freedom. The iSens® system simultaneously produced stimulation for sensation while recording high resolution muscle activity for real-time control. Although restored sensation did not significantly improve initial trials of prosthetic controller performance, the participant reported that sensation was helpful for functional tasks.
Conclusions: This case series describes a wirelessly connected, bidirectional neuroprosthetic system with somatosensory feedback and advanced myoelectric prosthetic control that is ready for implementation in long-term home use clinical trials.
Trial registration: ClinicalTrials.gov ID: NCT04430218, 2020-06-30.
Keywords: Implanted neural interfaces; Intramuscular electrodes; Myoelectric control; Neuroprosthesis; Peripheral nerve stimulation; Upper limb loss; Wireless communication.
© 2025. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Study volunteers provided written informed consent to participate in the study. All study procedures were approved by the VA Central IRB #19-34 (2020-05-04), the U.S. Food and Drug Administration (2020-01-21), and the Department of the Navy Human Research Protection Program #19-34 (2020-08-20). Consent for publication: No identifiable patient information was presented. Competing interests: DJT has patents on the C-FINE electrodes (US Patent #6456866B1). All other authors claim no competing interests for this work.
Figures



References
-
- Resnik L, Borgia M, Cancio J, Heckman J, Highsmith J, Levy C, et al. Dexterity, activity performance, disability, quality of life, and independence in upper limb Veteran prosthesis users: a normative study. Disabil Rehabil. 2022;44:2470–81. - PubMed
-
- Armstrong TW, Williamson MLC, Elliott TR, Jackson WT, Kearns NT, Ryan T. Psychological distress among persons with upper extremity limb loss. Br J Heal Psychol. 2019;24:746–63. - PubMed
-
- Kristjansdottir F, Dahlin LB, Rosberg H-E, Carlsson IK. Social participation in persons with upper limb amputation receiving an esthetic prosthesis. J Hand Ther. 2020;33:520–7. - PubMed
-
- Resnik L, Borgia M, Clark M. Function and quality of life of unilateral major upper limb amputees: effect of prosthesis use and type. Arch Phys Med Rehabil. 2020;101:1396–406. - PubMed
-
- Biddiss E, Chau T. Upper-limb prosthetics: critical factors in device abandonment. Am J Phys Med Rehab. 2007;86:977–87. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
