

Neurological outcomes and mortality following hyperoxemia in adult patients with acute brain injury: an updated meta-analysis and meta-regression
- PMID: 40270034
- PMCID: PMC12020189
- DOI: 10.1186/s13054-025-05387-7
Neurological outcomes and mortality following hyperoxemia in adult patients with acute brain injury: an updated meta-analysis and meta-regression
Abstract
Background: The aim of this study was to evaluate the association of arterial hyperoxemia with neurological outcomes and mortality in adults with acute brain injury (ABI).
Methods: Six electronic databases, including MEDLINE, Embase and online registers of clinical trials, were systematically searched from inception to June 1 st, 2024. Studies comparing the effects of hyperoxemia versus no hyperoxemia on outcomes of hospitalized adult patients with ABI-related conditions (e.g. traumatic brain injury, post-cardiac arrest, subarachnoid hemorrhage, intracerebral hemorrhage, and ischemic stroke) were included according to PRISMA guidelines. Data were pooled using a random-effects model for unadjusted and covariate-adjusted odds ratios. The primary outcome was poor neurological outcome as defined by each individual study, and the secondary outcome was all-cause mortality. Subgroup analyses were conducted based on principal diagnosis, timing of outcome measures, oxygenation thresholds, among other factors. Meta-regression was applied to identify sources of heterogeneity.
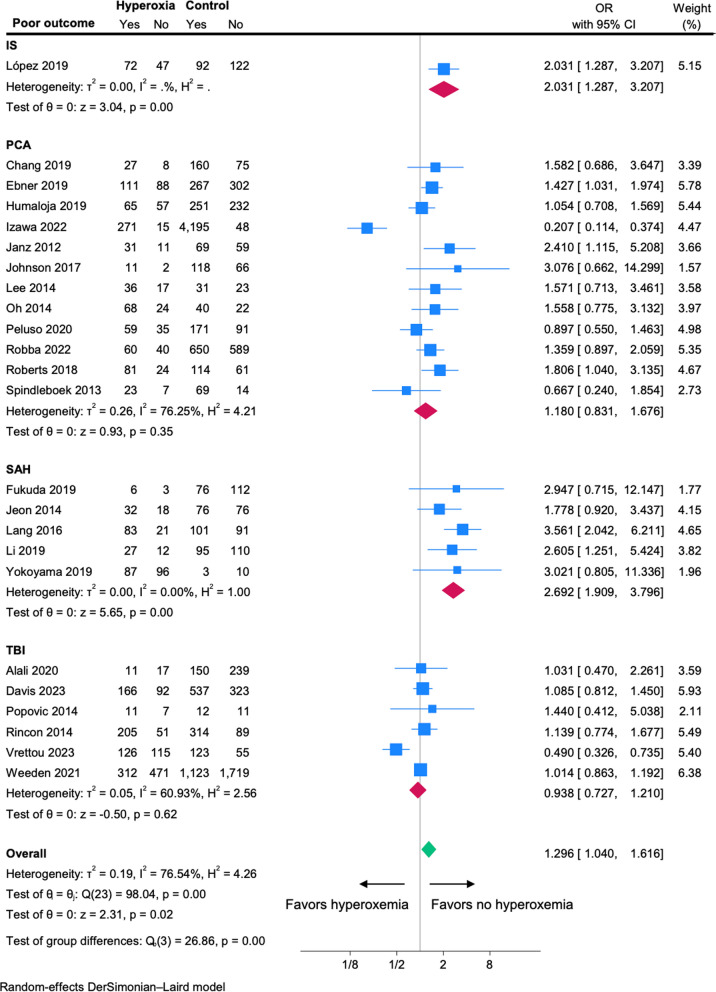
Results: After 7,849 nonduplicated records were screened, 66 studies fulfilled eligibility criteria for systematic review. The meta-analysis including 24 studies (16,635 patients) revealed that patients with hyperoxemia are 1.29 times more likely to develop poor neurological outcomes (unadjusted OR, 1.295; 95% Confidence Interval, CI 1.040-1.616) compared with those with no hyperoxemia, particularly in subarachnoid hemorrhage and ischemic stroke subgroups. The meta-analysis including 35 studies (98,207 patients) revealed that all-cause mortality is 1.13 times more likely (OR 1.13; 95% CI 1.002-1.282) in patients with hyperoxemia compared with no hyperoxemia.
Conclusions: In our study we found that hyperoxemia is significantly associated with an increased risk of poor neurological outcomes and mortality in patients with acute brain injury compared to those with no hyperoxemia. Our results suggest the importance of carefully adjusting oxygenation strategies in neurocritical ICUs.
Keywords: Acute brain injury; Hyperoxemia; Meta-analysis; Mortality; Neurological outcomes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



Comment in
-
Methodological considerations regarding cardiac arrest studies in hyperoxemia meta-analysis.Crit Care. 2025 Jun 17;29(1):245. doi: 10.1186/s13054-025-05500-w. Crit Care. 2025. PMID: 40528216 Free PMC article. No abstract available.
-
Hyperoxia and acute brain injury.Crit Care. 2025 Aug 21;29(1):377. doi: 10.1186/s13054-025-05618-x. Crit Care. 2025. PMID: 40841698 Free PMC article. No abstract available.
References
-
- Robba C, Battaglini D, Cinotti R, Asehnoune K, Stevens R, Taccone FS, et al. Individualized Thresholds of Hypoxemia and Hyperoxemia and their Effect on Outcome in Acute Brain Injured Patients: A Secondary Analysis of the ENIO Study. Neurocrit Care. 2023 Jun 15; - PubMed
-
- Carney N, Totten AM, O’Reilly C, Ullman JS, Hawryluk GWJ, Bell MJ, et al. Guidelines for the Management of Severe Traumatic Brain Injury. Fourth Edition Neurosurgery. 2017;80(1):6–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
