

Association of the Timing and Type of Acute Symptomatic Seizures With Poststroke Epilepsy and Mortality
- PMID: 40270248
- PMCID: PMC12180697
- DOI: 10.1161/STROKEAHA.124.050045
Association of the Timing and Type of Acute Symptomatic Seizures With Poststroke Epilepsy and Mortality
Abstract
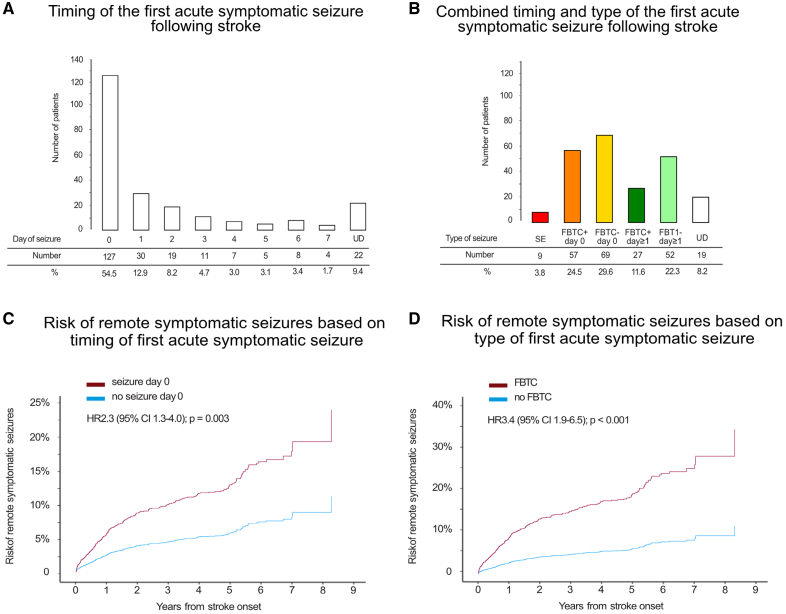
Background: Acute symptomatic seizures (ASyS) increase the risk of epilepsy and mortality after a stroke. The impact of the timing and type of ASyS remains unclear.
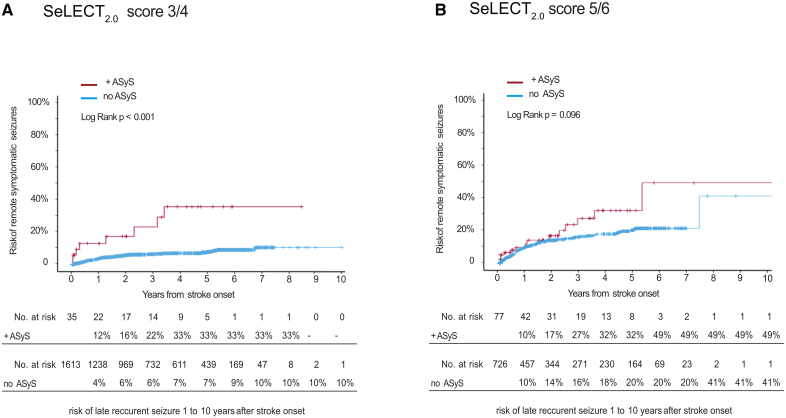
Methods: This multicenter cohort study included data from 9 centers between 2002 and 2018, with a final analysis in February 2024. The study included 4552 adults (2005 female; median age, 73 years) with ischemic stroke and no seizure history. Seizures were classified using International League Against Epilepsy definitions. We examined ASyS occurring within 7 days after stroke. The main outcomes were all-cause mortality and epilepsy. Validation of the updated SeLECT score (SeLECT-ASyS) was performed in 3 independent cohorts (Switzerland, Argentina, and Japan) collected between 2012 and 2024, including 74 adults with ASyS.
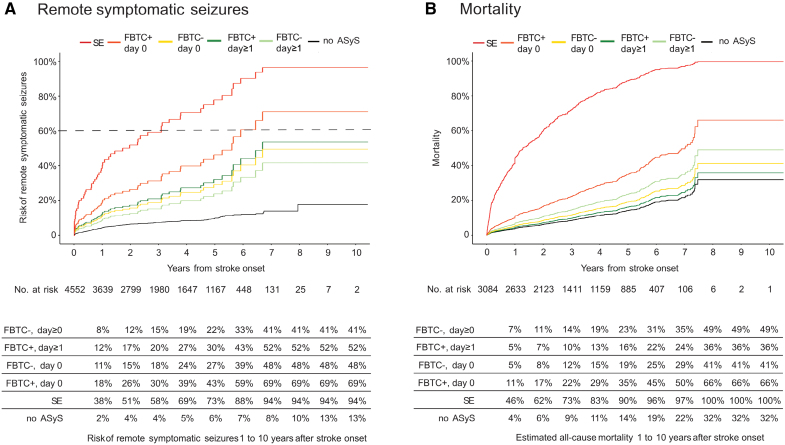
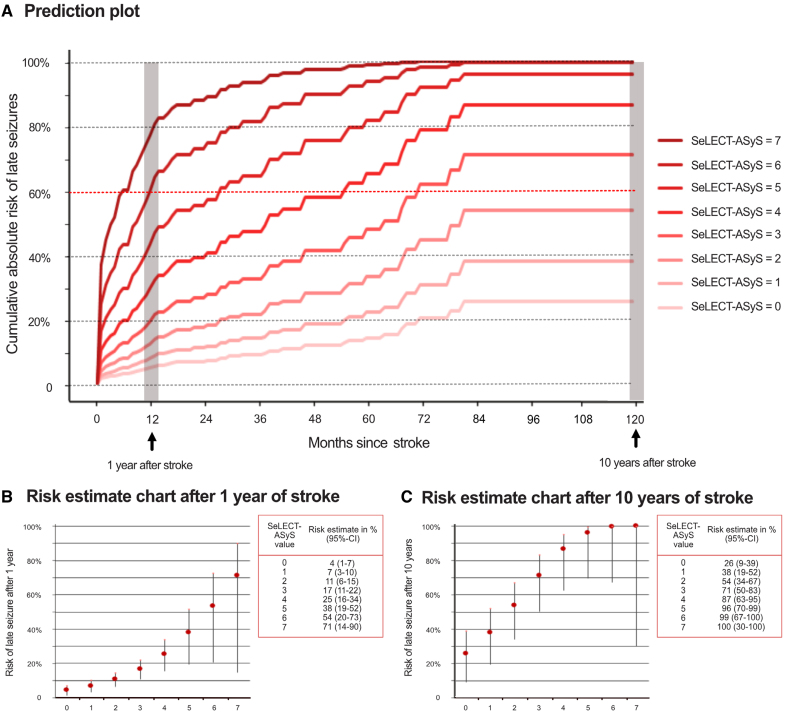
Results: The 10-year risk of poststroke epilepsy ranged from 41% to 94%, and mortality from 36% to 100%, depending on ASyS type and timing. ASyS on stroke onset day had a higher epilepsy risk (adjusted hazard ratio [aHR], 2.3 [95% CI, 1.3-4.0]; P=0.003) compared with later ASyS. Status epilepticus had the highest epilepsy risk (aHR, 9.6 [95% CI, 3.5-26.7]; P<0.001), followed by focal to bilateral tonic-clonic seizures (aHR, 3.4 [95% CI, 1.9-6.3]; P<0.001). Mortality was higher in those with ASyS presenting as focal to bilateral tonic-clonic seizures on day 0 (aHR, 2.8 [95% CI, 1.4-5.6]; P=0.004) and status epilepticus (aHR, 14.2 [95% CI, 3.5-58.8]; P<0.001). The updated SeLECT-ASyS model, available as an application, outperformed a previous model in the derivation cohort (concordance statistics, 0.68 versus 0.58; P=0.02) and in the validation cohort (0.70 versus 0.50; P=0.18).
Conclusions: ASyS timing and type significantly affect epilepsy and mortality risk after stroke, improving epilepsy prediction and guiding patient counseling.
Keywords: epilepsy; ischemic stroke; seizures; status epilepticus; stroke.
Conflict of interest statement
Dr Abraira reports travel support from Angelini Pharma; compensation from Union Chimique Belge for consultant services and Jazz Pharmaceuticals for other services; and travel support from Jazz Pharmaceuticals. Dr von Oertzen reports grants from the Austrian Science Fund; and compensation from UCB GmBH for other services. Dr Wagner reports compensation from Union Chimique Belge, Pfizer, and Janssen Cilag (Europe, Middle East, and Africa) for other services; compensation from Janssen Cilag EMEA for consultant services; compensation from Boehringer Ingelheim for other services; travel support from Boehringer Ingelheim, Novartis, and Janssen Cilag (Europe, Middle East and Africa); compensation from AstraZeneca for other services; and Novartis for consultant services. J.S. Duncan reports grants from Wellcome Trust. J.W. Sander reports compensation from The
Figures
References
-
- Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota: 1935-1984. Epilepsia. 1993;34:453–468. doi: 10.1111/j.1528-1157.1993.tb02586.x - PubMed
-
- Sinka L, Abraira L, Imbach LL, Zieglgansberger D, Santamarina E, Alvarez-Sabin J, Ferreira-Atuesta C, Katan M, Scherrer N, Bicciato G, et al. Association of mortality and risk of epilepsy with type of acute symptomatic seizure after ischemic stroke and an updated prognostic model. JAMA Neurol. 2023;80:605–613. doi: 10.1001/jamaneurol.2023.0611 - PMC - PubMed
-
- Beghi E, D’Alessandro R, Beretta S, Consoli D, Crespi V, Delaj L, Gandolfo C, Greco G, La Neve A, Manfredi M, et al. ; Epistroke Group. Incidence and predictors of acute symptomatic seizures after stroke. Neurology. 2011;77:1785–1793. doi: 10.1212/WNL.0b013e3182364878 - PubMed
-
- Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, Engel J, Jr, Forsgren L, French JA, Glynn M, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. 2014;55:475–482. doi: 10.1111/epi.12550 - PubMed
