

Challenges and opportunities to minimize the dose in the neurovascular bundles during prostate radiotherapy
- PMID: 40270948
- PMCID: PMC12018000
- DOI: 10.1016/j.ctro.2025.100959
Challenges and opportunities to minimize the dose in the neurovascular bundles during prostate radiotherapy
Abstract
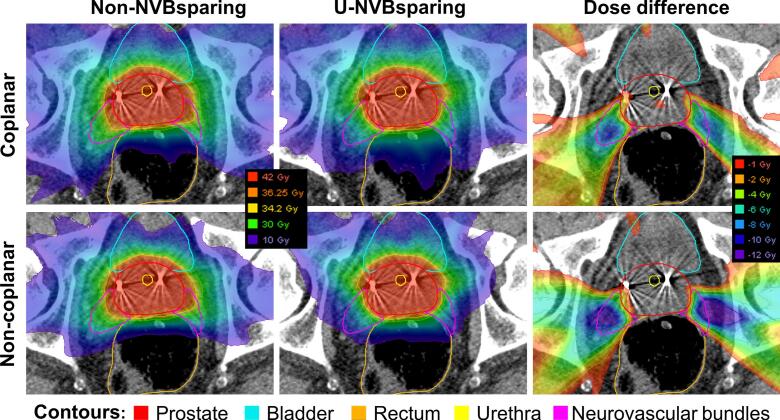
Background and purpose: Radiation damage to the neurovascular bundles (NVB) has been linked to erectile dysfunction after prostate cancer radiotherapy (PCa). NVB sparing using coplanar and non-coplanar automated treatment planning is presented here in two settings: (1) without compromising target coverage, (2) allowing target coverage compromise.
Material and methods: 20 previously treated patients with localized PCa. Based on a MRI-CT match, the NVB were retrospectively delineated. All treatment plans (5 × 7.25 Gy) were automatically generated using Erasmus-iCycle (in-house automated treatment planning algorithm). Non-NVB sparing (non-NVBsparing) plans and NVB sparing plans in two settings were generated: (1) uncompromised NVB sparing (u-NVBsparing; maintaining target coverage) (2) and compromised NVB sparing (c-NVBsparing; allowing target underdosage). Coplanar and non-coplanar beam arrangements were compared. U-NVBsparing was compared to non-NVBsparing. C-NVBsparing plans were visualized in Pareto fronts. Statistical significance (p-value < 0.05) was determined by Wilcoxon signed-rank test.
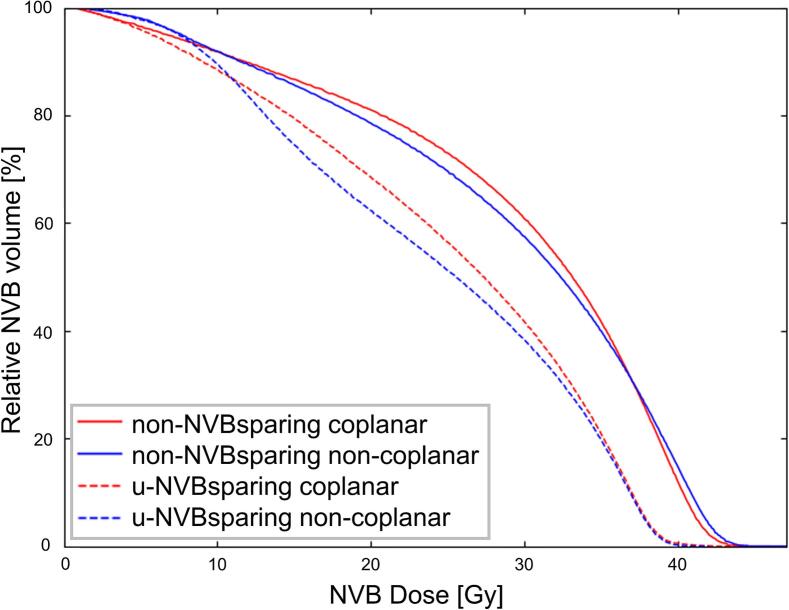
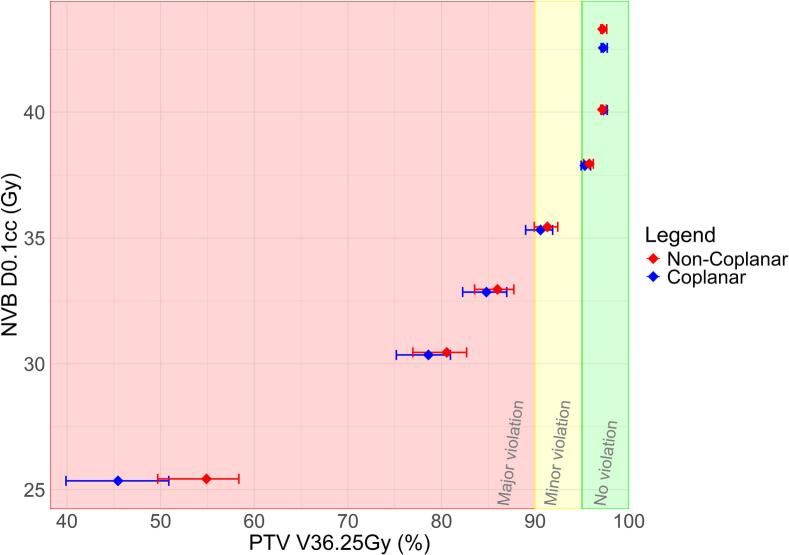
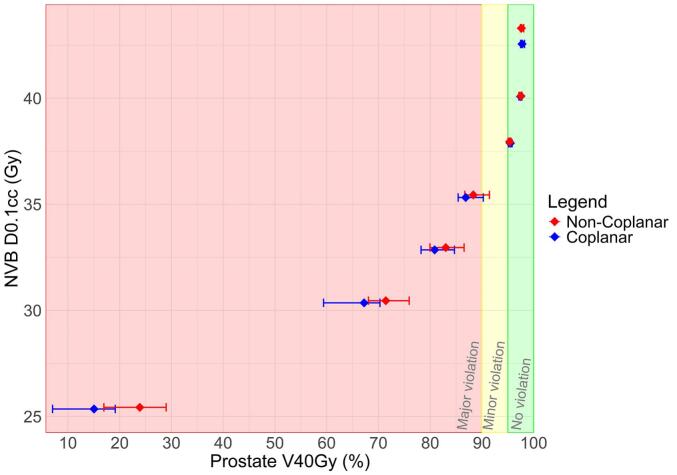
Results: u-NVBsparing compared to non-NVBsparing plans showed statistically significant median reductions in NVB D0.1 cc (38.9 vs 42.6 Gy for coplanar; 38.9 vs 43.3 Gy for non-coplanar) and Dmean (25.6 vs 30.0 Gy for coplanar; 24.7 vs 30.2 Gy for noncoplanar). Further lowering NVB D0.1 cc in c-NVBsparing plans clearly correlated to lower target coverage. Non-coplanar c-NVBsparing plans maintained significantly higher target coverages for similar NVB D0.1 cc values, compared to coplanar plans.
Conclusion: NVB sparing without compromising target coverage is feasible. No clinically relevant benefit was found for non-coplanar compared to coplanar NVB sparing plans, although overall statistically superior. Further sparing of the NVB comes at the cost of target coverage, for which a Pareto front could be used as a tool in clinical practise.
Keywords: Erectile dysfunction; Neurovascular bundle; Prostate cancer; SBRT; Treatment planning.
© 2025 The Authors. Published by Elsevier B.V. on behalf of European Society for Radiotherapy and Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Mottet N., Bellmunt J., Bolla M., Briers E., Cumberbatch M.G., De Santis M., et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol. 2017;71:618–629. - PubMed
-
- Loi M., Wortel R.C., Francolini G., Incrocci L. Sexual Function in Patients Treated With Stereotactic Radiotherapy For Prostate Cancer: A Systematic Review of the Current Evidence. J Sex Med. 2019;16:1409–1420. - PubMed
-
- Hall W.A., Deshmukh S., Bruner D.W., Michalski J.M., Purdy J.A., Bosch W., et al. Quality of life implications of dose-escalated external beam radiation for localized prostate cancer: Results of a prospective randomized phase 3 clinical trial, NRG/RTOG 0126. International Journal of Radiation Oncology* Biology*. Physics. 2022;112:83–92. - PMC - PubMed
-
- Sanda M.G., Dunn R.L., Michalski J., Sandler H.M., Northouse L., Hembroff L., et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. N Engl J Med. 2008;358:1250–1261. - PubMed
-
- Nolan M.W., Marolf A.J., Ehrhart E.J., Rao S., Kraft S.L., Engel S., et al. Pudendal nerve and internal pudendal artery damage may contribute to radiation-induced erectile dysfunction. International Journal of Radiation Oncology* Biology*. Physics. 2015;91:796–806. - PubMed
LinkOut - more resources
Full Text Sources
