

Editorial
doi: 10.1007/s00404-025-08027-1.
Epub 2025 Apr 24.
Pattern recognition for prenatal diagnosis of a parachute mitral valve
Affiliations
- PMID: 40274665
- PMCID: PMC12334449
- DOI: 10.1007/s00404-025-08027-1
Item in Clipboard
Editorial
Pattern recognition for prenatal diagnosis of a parachute mitral valve
Arch Gynecol Obstet.
2025 Aug.
No abstract available
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests. Ethical approval: All the patients have given written informed approval for data collection, analysis and the use of these for research. As the Ethics Committee of the University of Bonn does not request formal approval for an anonymized retrospective analysis of clinical data, ethical consent was not required. Consent to participate: Informed consent was obtained from every patient participating in this review for clinical data collection, analysis and the use of those data for research. Consent for publication: Consent for publication was obtained from every patient participating in this review.
Figures

Prenatal sonographic examination of a parachute mitral valve (PMV) (a–e) in comparison to a normal mitral valve (MV) (f–j); a four chamber-view of the fetus at 20 + 4 weeks of GA displaying disproportions of the left heart structures compared to right heart-sided structures (RA > LA width in systole; RV > LV; RV 5.4 mm, + 1.19 z-score; LV: 4.2 mm,− 1.6 z-score), as associations to LVOT obstructions are frequently seen. a, b Same fetus with the four chamber-view showing the extreme narrow mitral orifice, typically eccentric (3.1 mm, − 4.8 z-score; TV/MV ratio: 1.9). In diastole, the redundant anterior chords fold over on themselves, appearing as swirling echogenic patterns in the LV (dotted arrow in b). Further, the typical paradoxical movement of the interventricular septum bowing into the perimembranous part of the interventricular septum is demonstrated (continuous arrow in b). c, d Parasternal short-axis view demonstrating typical aspects of the single papillary muscle (dotted circle in c) of the mitral valve, with a restricted opening (dotted circle in d). e Echocardiographic parasternal long-axis view showing a single papillary muscle inserting to the leaflets by short and thickened chordae tendineae (arrow). f–j Normal findings of an unsuspicious MV. f, g Four chamber-view with an unsuspicious LV:RV proportion; normal centrally positioned mitral orifice and an absent excursion of the IVS in diastole. h, i Parasternal short-axis view at the mitral valve level showing both papillary muscle groups (posteromedial papillary muscle (PMPM) and anterolateral papillary muscle (ALPM) with an unrestricted orifice appearing as a “fish mouth”, demonstrating a not restricted opening of the valve. j Regular parasternal long-axis view showing unsuspicious chordae tendineae (arrow). LA left atrium, LV left ventricle, MV
mitral valve, PMPM posteromedial papillary muscle, RA right atrium, RV right ventricle
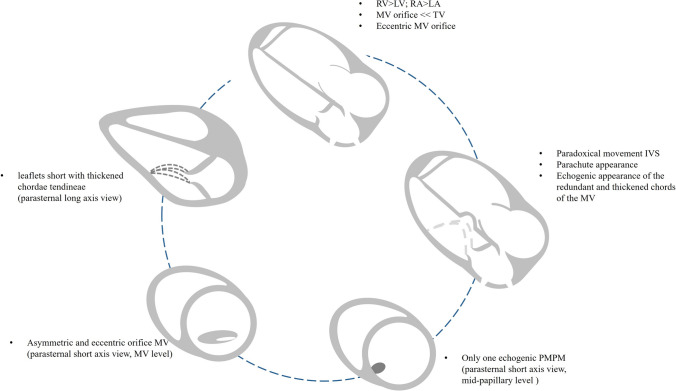
Diagnostic algorithm for prenatal suspected parachute mitral valve. IVS interventricular septum, LA left atrium, LV left ventricle, MV mitral valve, PMPM posteromedial papillary muscle, RA right atrium, RV right ventricle, TV tricuspid valve
References
-
- Oosthoek PW, Wenink AC, Wisse LJ, Gittenberger-de Groot AC (1998) Development of the papillary muscles of the mitral valve: morphogenetic background of parachute-like asymmetric mitral valves and other mitral valve anomalies. J Thorac Cardiovasc Surg 116:36–46. 10.1016/S0022-5223(98)70240-5 - DOI - PubMed
-
- Carpentier A, Branchini B, Cour JC et al (1976) Congenital malformations of the mitral valve in children. Pathology and surgical treatment. J Thorac Cardiovasc Surg 72:854–866 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
