

Assessing Tocolytic Potency: Variability and Accuracy of AUC Versus Amplitude-Based Assessment of Pregnant Human Myometrial Contractions Ex Vivo
- PMID: 40274731
- PMCID: PMC12187858
- DOI: 10.1007/s43032-025-01864-0
Assessing Tocolytic Potency: Variability and Accuracy of AUC Versus Amplitude-Based Assessment of Pregnant Human Myometrial Contractions Ex Vivo
Abstract
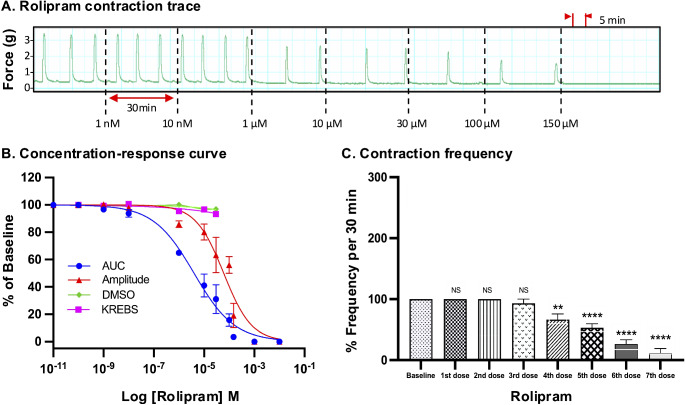
The methodological approaches used to evaluate the inhibitory effects (potency determination) of tocolytic agents on human uterine contractions in ex vivo systems vary, and none of the methodologies has been subjected to scrutiny in terms of objectivity, variability, and reliability. Therefore, this study aimed to assess and compare the reliability of using area under the curve (AUC) versus amplitude alone-based assessment of contraction traces to generate concentration-response curves, which were then used to calculate the tocolytic concentrations that inhibited 25% (IC25) and 50% (IC50) of baseline contractility. The accuracy of the determined inhibitory concentrations (IC) was then scrutinized while taking into consideration the contraction parameters (amplitude, frequency, duration) affected by the different tocolytics. To do this, pregnant human myometrial strips (term, not-in-labor) were treated with cumulative concentrations of the contraction-blocking agents, nifedipine (NIF), indomethacin (IND), 2-aminoethoxydiphenyl borate (2-APB), glycyl-h-1152 (GH), aminophylline (AMP), or rolipram (ROL)). Concentration-response curves were generated using either AUC or amplitude alone as the index of contraction inhibition, from which tocolytic IC25 and IC50 concentrations were calculated and compared (i.e. IC25(AUC) vs. IC25(Amplitude)). The effects of each tocolytic on contraction frequency were also quantified. To assess accuracy, each tocolytic was applied to contracting strips as a single treatment at their respective IC25(AUC/Amplitude) and IC50(AUC/Amplitude), and then the inhibitory effect re-quantified against both contraction AUC and amplitude alone. Significant differences between IC50(AUC) and IC50(Amplitude) were detected for AMP (318.5 vs. 450 µM), ROL (4.3 vs. 55 µM), and IND (59.5 vs. 75 µM), whereas AUC versus amplitude-based IC50 concentrations were comparable for NIF (10 vs. 10 nM), GH (18.2 vs. 15 µM), and 2-APB (53 vs. 57 µM). Similarly, the determined IC25(AUC) and IC25(Amplitude) were again significantly different for AMP (175 vs. 277 µM), ROL (515 nM vs. 15 µM), and IND (28 vs. 42 µM), but also for 2-APB (27 vs. 40 µM). The confirmation studies revealed that a single dose of the tocolytics at their determined IC25(AUC) and IC50(AUC) concentrations consistently reduced contraction AUC by approximately 25% and 50%, respectively, whereas single doses of the IC25(Amplitude) and IC50(Amplitude) concentrations revealed inconsistent results. Of the six tocolytics, four reduced contraction amplitude by > 25% when applied as a single dose at IC25(Amplitude), while three reduced contraction amplitude by > 50% when applied at IC50(Amplitude). Our experimental data indicate that when determining tocolytic potency, assessment of ex vivo contraction traces via AUC is more accurate and consistent than assessment via amplitude alone. Our study finds that whilst tocolytics that increase contraction frequency (while decreasing amplitude) can be assessed by either AUC or amplitude-based determination, tocolytics that either significantly reduce or largely do not affect contraction frequency should only be analyzed via AUC.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical Approval: The study was approved by the Hunter and New England Area Human Research Ethics Committee (2019/ETH12330). Consent to Participate: All participants gave informed written consent. Consent for Publication: Not applicable. Persons: We are grateful to the pregnant women who donated myometrial samples, to our research midwife, Ms. Anne Wright, and acknowledge the help of the Obstetrics, Midwifery, and Surgical staff at the John Hunter Hospital, Newcastle. Competing Interests: The authors declare that they have no competing interests.
Figures











References
-
- Chawanpaiboon S, Vogel JP, Moller A-B, Lumbiganon P, Petzold M, Hogan D, Landoulsi S, Jampathong N, Kongwattanakul K, Laopaiboon M, Lewis C, Rattanakanokchai S, Teng DN, Thinkhamrop J, Watananirun K, Zhang J, Zhou W, Gülmezoglu AM. Global, regional, and National estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Global Health. 2019;7:e137–46. 10.1016/S2214-109X(18)30451-0. - PMC - PubMed
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet (London England). 2008;371:9608:261–9. 10.1016/s0140-6736(08)60136-1. - PubMed
-
- Khan KA, Petrou S, Dritsaki M, Johnson SJ, Manktelow B, Draper ES, Smith LK, Seaton SE, Marlow N, Dorling J, Field DJ, Boyle EM. Economic costs associated with moderate and late preterm birth: a prospective population-based study. BJOG: Int J Obstet Gynecol. 2015;122:11. 10.1111/1471-0528.13515. - PubMed
-
- Petrou S, Yiu HH, Kwon J. Economic consequences of preterm birth: a systematic review of the recent literature (2009–2017). Arch Dis Child. 2019;104:5456. 10.1136/archdischild-2018-315778. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
