

Neurocognitive resilience as a predictor of psychosis onset and functional outcomes in individuals at high risk
- PMID: 40275324
- PMCID: PMC12023670
- DOI: 10.1186/s12916-025-04059-1
Neurocognitive resilience as a predictor of psychosis onset and functional outcomes in individuals at high risk
Abstract
Background: Neurocognitive resilience (NCR) refers to the ability of individuals to maintain cognitive function despite the presence of risk factors for psychosis. Investigating NCR is important as it may help predict the onset of psychosis and functional outcomes in individuals at clinical high risk (CHR) for psychosis.
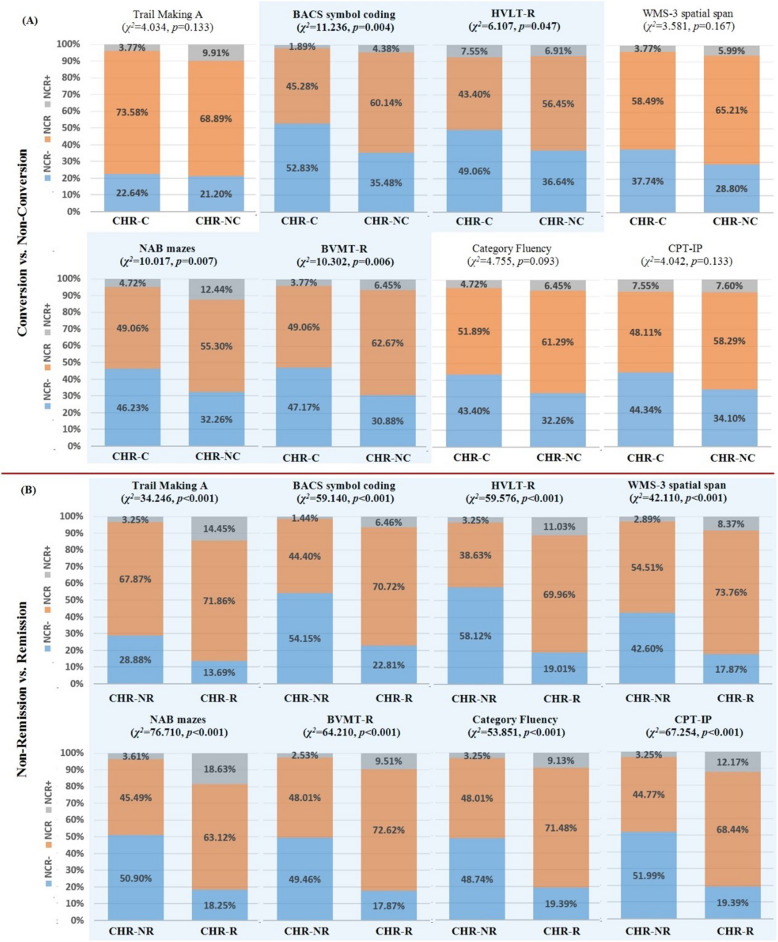
Methods: This study employed a multi-group prospective design with a 3-year follow-up as part of the ShangHai At Risk for Psychosis-Extended project. Neurocognitive performance was assessed using the Chinese version of the Measurement and Treatment Research to Improve Cognition in Schizophrenia Consensus Cognitive Battery. The study focused on two primary outcomes: conversion/non-conversion to psychosis (CHR-C/CHR-NC) and non-remission/remission (CHR-NR/CHR-R). NCR was defined based on the adjusted cognitive variable relative to the healthy control(HC) group's mean, with three categories: NCR (NCR = 0) for scores within one standard deviation, NCR + (NCR = 1) for scores more than one standard deviation above, and NCR - (NCR = - 1) for scores more than one standard deviation below.
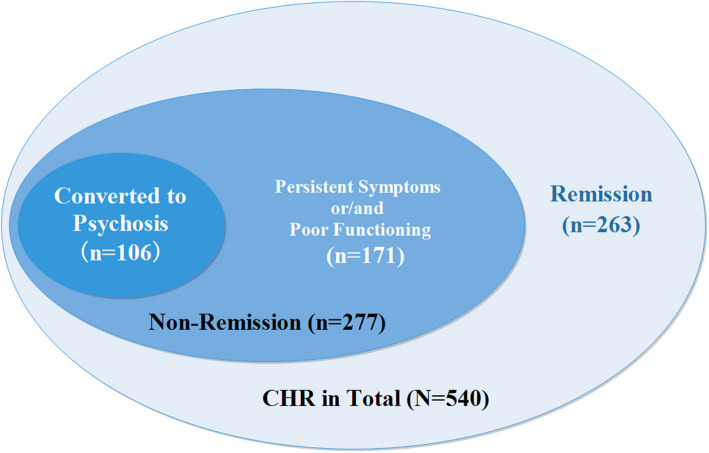
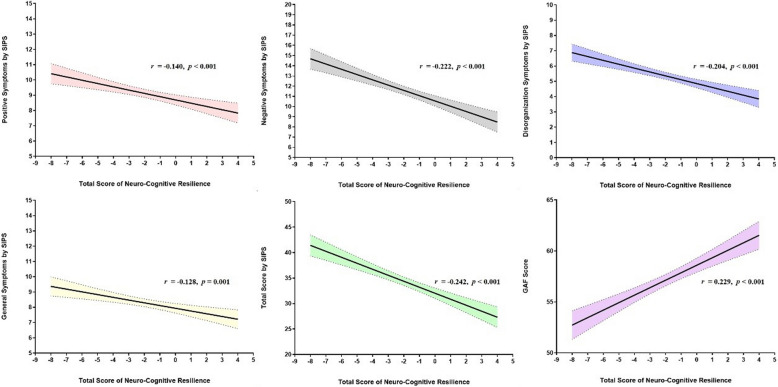
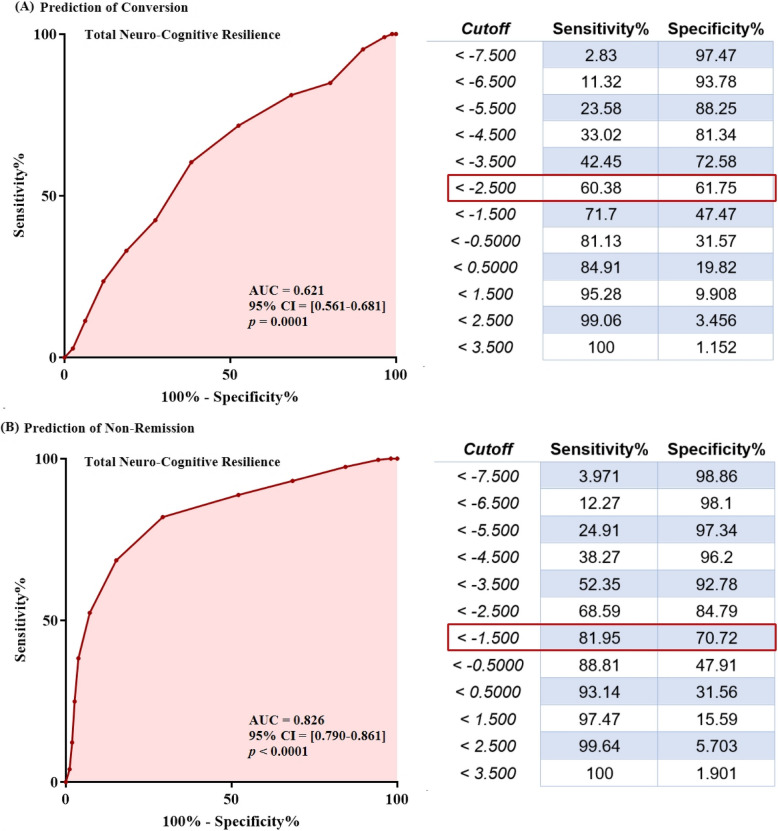
Results: The study included 771 individuals at CHR (346 males, mean age 18.8 years) and 764 HCs (359 males, mean age 22.5 years). Among the CHR participants, 540 (70.0%) completed the 3-year follow-up, with 106 (19.6%) converting to psychosis (CHR-C) and 277 (51.3%) classified as non-remission (CHR-NR). Significant negative correlations were found between the total NCR score and various clinical symptoms. Comparing CHR-C and non-converters (CHR-NC), there were notable differences in NCR distributions across four cognitive measures, with a higher proportion of CHR-C individuals categorized as NCR - . For CHR-NR versus remission (CHR-R), CHR-NR individuals were more likely to be classified as NCR - across nearly all cognitive domains. The receiver operating characteristic (ROC) curve for predicting conversion to psychosis yielded an area under the curve (AUC) of 0.621 (95% CI (0.561-0.681), p = 0.0001), while the ROC for predicting non-remission demonstrated a higher AUC of 0.826 (95% CI (0.790-0.861), p < 0.0001).
Conclusions: NCR was associated with both conversion to psychosis and non-remission outcomes in CHR individuals, showing notable predictive accuracy, particularly for non-remission.
Keywords: Cognition; Functional outcome; Prodromal psychosis; Remission; Transition; Ultra high risk.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for the research (including the consent procedure) was granted by the Institutional Review Board of the Shanghai Mental Health Center (IRB2016-009). All participants provided written consent to be involved in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Models of mild cognitive deficits in risk assessment in early psychosis.Psychol Med. 2024 Jul;54(9):2230-2241. doi: 10.1017/S0033291724000382. Epub 2024 Mar 4. Psychol Med. 2024. PMID: 38433595
-
Association of Neurocognition With Transition to Psychosis: Baseline Functioning in the Second Phase of the North American Prodrome Longitudinal Study.JAMA Psychiatry. 2016 Dec 1;73(12):1239-1248. doi: 10.1001/jamapsychiatry.2016.2479. JAMA Psychiatry. 2016. PMID: 27806157 Free PMC article.
-
Associations between age and neurocognition in individuals at clinical high risk and first-episode psychosis.Psychiatry Res. 2023 Sep;327:115385. doi: 10.1016/j.psychres.2023.115385. Epub 2023 Jul 27. Psychiatry Res. 2023. PMID: 37567111
-
Neurocognition in clinical high risk young adults who did or did not convert to a first schizophrenic psychosis: a meta-analysis.Schizophr Res. 2013 Sep;149(1-3):48-55. doi: 10.1016/j.schres.2013.06.017. Epub 2013 Jul 5. Schizophr Res. 2013. PMID: 23830855 Review.
-
P300 as an index of transition to psychosis and of remission: Data from a clinical high risk for psychosis study and review of literature.Schizophr Res. 2020 Dec;226:74-83. doi: 10.1016/j.schres.2019.02.014. Epub 2019 Feb 25. Schizophr Res. 2020. PMID: 30819593 Free PMC article. Review.
Cited by
-
Gender differences in neurocognitive impairment among first-episode, drug-naïve schizophrenia patients: a cross-sectional study.Front Psychiatry. 2025 Aug 4;16:1642291. doi: 10.3389/fpsyt.2025.1642291. eCollection 2025. Front Psychiatry. 2025. PMID: 40831523 Free PMC article.
References
-
- Yung AR, McGorry PD, McFarlane CA, Jackson HJ, Patton GC, Rakkar A. Monitoring and care of young people at incipient risk of psychosis. Schizophr Bull. 1996;22(2):283–303. - PubMed
-
- Yung AR, Yuen HP, McGorry PD, Phillips LJ, Kelly D, Dell’Olio M, et al. Mapping the onset of psychosis: the Comprehensive Assessment of At-Risk Mental States. Aust N Z J Psychiatry. 2005;39(11–12):964–71. - PubMed
-
- Cui H, Giuliano AJ, Zhang T, Xu L, Wei Y, Tang Y, et al. Cognitive dysfunction in a psychotropic medication-naive, clinical high-risk sample from the ShangHai-At-Risk-for-Psychosis (SHARP) study: Associations with clinical outcomes. Schizophr Res. 2020;226:138–46. - PubMed
MeSH terms
Grants and funding
- 2023YFC2506800/Ministry of Science and Technology of the People's Republic of China
- 82171544, 82371505, 82151314, 82101623/National Natural Science Foundation of China
- 82171544, 82371505, 82151314, 82101623/National Natural Science Foundation of China
- JCYJ20220530165009020/Shenzhen Science and Technology Plan Project
- SZSM202011014/Shenzhen Medical and Health Three Project
LinkOut - more resources
Full Text Sources
Medical
