

Global frequency, diagnosis, and treatment of hereditary angioedema with normal C1 inhibitor
- PMID: 40276547
- PMCID: PMC12020835
- DOI: 10.1016/j.jacig.2025.100446
Global frequency, diagnosis, and treatment of hereditary angioedema with normal C1 inhibitor
Abstract
Background: Hereditary angioedema (HAE) is a rare genetic disease, most frequently associated with deficiency or dysfunction in the C1 inhibitor protein. HAE with normal C1 inhibitor (HAE-nC1INH) lacks standardized diagnostic tests, limiting precise prevalence estimates and development of specific treatment guidelines.
Objective: This study sought to describe the global frequency, diagnostic pathway, and current treatment patterns of HAE-nC1INH.
Methods: Board-certified HAE-treating physicians from accredited Angioedema Centers of Reference and Excellence (ACAREs) were invited to complete a 27-item online survey between December 2022 and April 2023.
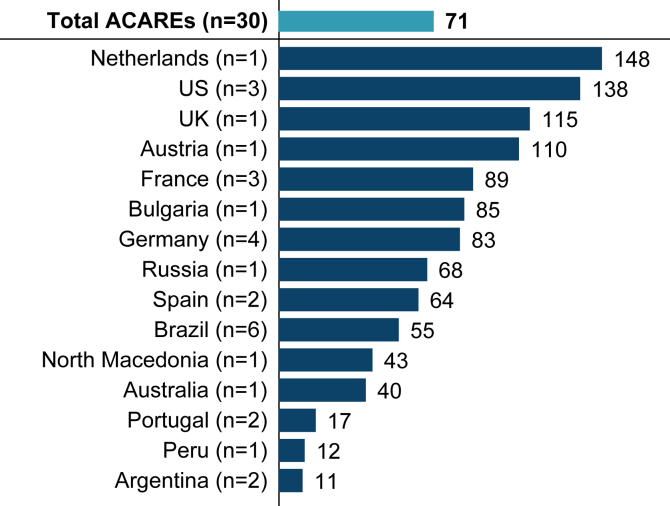
Results: Thirty physicians from 30 ACAREs across 15 countries reported a mean of 71 (range, 11-148) patients with HAE assessed/treated within the previous 12 months. On average, physicians estimated 24% (range, 2-44%) of patients with HAE were diagnosed with HAE-nC1INH, most of whom were adults (88%). To diagnose HAE-nC1INH, physicians most commonly assessed family history and plasma C4 levels (90% each), and C1 function and quantitative levels (87% each). On-demand and prophylactic treatment patterns varied widely across countries, with an average (range) of 56% (33-100%) of patients receiving on-demand treatment only, and 37% (0-67%) receiving both on-demand and prophylactic treatment. Physicians identified the greatest unmet needs in HAE-nC1INH management as treatment specifically indicated for this patient population and availability of an oral treatment.
Conclusion: HAE-nC1INH may be more prevalent than previously reported. Importantly, our findings revealed varying diagnostic and treatment approaches. Validated, accessible diagnostic biomarkers and clinical outcomes derived from rigorous clinical trials assessing mechanistically based treatments would advance understanding and management of HAE-nC1INH.
Keywords: Hereditary angioedema; diagnostics; management; normal C1INH; prevalence; treatment.
© 2025 The Authors.
Conflict of interest statement
Sponsored and funded by 10.13039/100031004KalVista Pharmaceuticals and conducted in collaboration with ACARE. KalVista participated in the design and conduct of the study. Statistical analyses were conducted by Outcome Insights, funded by 10.13039/100031004KalVista. The initial draft of the report was prepared by a medical writer funded by KalVista. Subsequent revisions and the final decision to submit the report for publication were made by the authors, who vouch for the accuracy and completeness of the data and for the fidelity of the study to the protocol. Data-sharing statement: KalVista Pharmaceuticals accepts requests from qualified researchers who wish to access clinical trial data and associated information, such as Clinical Study Reports (CSRs) with appropriately redacted appendices to protect participant privacy. Inquiries may be directed to DSP@kalvista.com. Disclosure of potential conflict of interest: M. Magerl received personal fees/nonfinancial support from Astria, Shire/Takeda, CSL Behring, Pharming, BioCryst, KalVista Pharmaceuticals, Pharvaris, Ionis, Intellia, and Octapharma. M. Riedl is or recently was a speaker and/or advisor for and/or has received research funding from Astria, BioCryst, BioMarin, Celldex, CSL Behring, Cycle Pharma, Grifols, Intellia, Ionis, KalVista, Pfizer, Pharming, Pharvaris, Sanofi-Regeneron, and Takeda. A. Bauer received personal fees and/or other support from BioCryst, CSL Behring, and Takeda. J. A. Bernstein has received grants and/or honoraria from KalVista, BioCryst, BioMarin, CSL Behring, Intellia, Ionis, Pharming, Pharvaris, and Shire/Takeda; and serves as immediate past president of the American Academy of Allergy, Asthma & Immunology. L. Bouillet has consulted/served as speaker for, engaged in research and educational projects with, and/or accepted travel grants from BioCryst, CSL Behring, Takeda, KalVista, Pharvaris, and Intellia. M. S. Buckland is or recently was a speaker and/or advisor for and/or has received research funding from BioCryst, CSL Behring, Pharming, and Takeda. T. Buttgereit is or recently was a speaker and/or advisor for and/or has received research funding from Aquestive, BioCryst, CSL Behring, GSK, Hexal, KalVista, Medac, Novartis, Pharming, Pharvaris, Roche, Sanofi-Aventis, Swixx BioPharma, and Takeda. D. M. Cohn has received consulting fees paid to the institution, honoraria paid to the institution, meeting/travel support, research support, and/or served on advisory boards from KalVista, Astria, BioCryst, CSL Behring, Intellia, Ionis Pharmaceuticals, Pharming, Pharvaris, and Takeda; and serves a leadership role in the HAE International medical advisory panel for Central Eastern Europe and Benelux. T. Craig reports research with BioMarin, KalVista, Pharvaris, GSK, CSL Behring, Takeda, Ionis, Intellia, Astra, Pfizer, Regeneron and Grifols; speaker for Takeda, CSL Behring, and Grifols; and consultant for BioMarin, Intellia, CSL Behring, Takeda, BioMarin, Ionis, Astra, KalVista, and BioCryst; has Center designations from the International Hereditary Angioedema Association and Alpha-1 Foundation; and is a member of the medical advisory board for the HAE-A. R. F. Criado has received grants, personal fees, and/or nonfinancial support from Amgen, Lilly, Novartis, and Pfizer. A. Du-Thanh has received meeting/travel support, research support, and/or served on advisory boards for BioCryst, Novartis, Pharvaris, and Takeda. O. Fain has received personal fees from Behring, BioCryst, KalVista, and Takeda; and a grant from BioCryst. M. Gonçalo has participated as speaker/advisor and/or received department research funding from AbbVie, Almirall, AstraZeneca, Elli-Lilly, LEO Pharmaceutica, Pfizer, Sanofi, Novartis, and Takeda. J. Greve is or recently was a speaker and/or advisor for and/or has received research funding from BioCryst, CSL Behring, KalVista, and Takeda. A. S. Grumach receives research funding from the Brazilian National Council for Scientific and Technological Development (CNPq) and a grant of researcher initiative from Shire/Takeda; and is or recently was a speaker and/or advisor for Catalyst Pharmaceuticals, CSL Behring, Takeda, KalVista, Pharvaris, Pint-Pharma, and MultiCare. M. Guilarte is or recently was a speaker and/or advisor for and/or has received research funding from BioCryst, CSL Behring, KalVista, Pharvaris, and Takeda. C. Katelaris has received personal fees from AstraZeneca, CSL Behring, GSK, KalVista, Pharvaris, and Sanofi. T. Kinaciyan is or recently was a speaker and/or advisor for and/or has received research funding from BioCryst, CSL Behring, KalVista, KINIKSA, Novartis, Pharvaris, Sanofi-Aventis, and Takeda. E. A. Latysheva has received personal fees from CSL Behring, Octapharma, Novartis, and Takeda; and a grant from Takeda. R. Lleonart has received consulting fees, honoraria, payment for expert testimony, meeting/travel support, and/or served on advisory boards for KalVista, BioCryst, CSL Behring, Pharming, and Takeda. E. Mansour has received grants and/or personal fees from AstraZeneca, CSL Behring, GSK, Novartis, Sanofi, and Takeda. V. Grivcheva-Panovska has served on advisory boards for CSL Behring, Takeda, BioCryst, KalVista, and Pharvaris; and has received honoraria for presentations from CSL Behring and Takeda, an unrestricted research grant from CSL Behring, and travel assistance from CSL Behring. A. Spínola Santos has received personal fees from BioCryst, CSL Behring, Diater Laboratorio de Diagnóstico y Aplicaciones SA, and Takeda. P. Staubach has received grants and/or consulting fees from Novartis, CSL Behring, Sanofi, Takeda, KalVista, BioCryst, and Pharvaris. A. Valerieva has received honoraria for educational lectures, acted as consultant for, and/or has received sponsorship for educational meetings and/or research projects from Shire/Takeda, Pharming Group NV, CSL Behring, SOBI, AstraZeneca, Berlin-Chemie/Menarini Group, Teva, Novartis, Ewopharma, Stellergenes-Greer, Pharvaris, KalVista, Ionis, Astria, and Organon. S. Danese and J. Ulloa received consulting fees from KalVista. P. K. Audhya is an employee of KalVista. M. Maurer was a speaker and/or advisor for and/or received research funding from Astria, BioCryst, CSL Behring, Intellia, Ionis, KalVista, Pharvaris, and Takeda. The rest of the authors declare that they have no relevant conflicts of interest.
Figures





References
-
- Busse P.J., Christiansen S.C., Riedl M.A., Banerji A., Bernstein J.A., Castaldo A.J., et al. US HAEA Medical Advisory Board 2020 guidelines for the management of hereditary angioedema. J Allergy Clin Immunol Pract. 2021;9:132–150.e3. - PubMed
-
- Maurer M., Magerl M., Betschel S., Aberer W., Ansotegui I.J., Aygoren-Pursun E., et al. The international WAO/EAACI guideline for the management of hereditary angioedema—the 2021 revision and update. Allergy. 2022;77:1961–1990. - PubMed
-
- Lumry W.R., Settipane R.A. Hereditary angioedema: epidemiology and burden of disease. Allergy Asthma Proc. 2020;41:S08–S13. - PubMed
-
- Christiansen S.C., Wilmot J., Castaldo A.J., Zuraw B.L. The US Hereditary Angioedema Association Scientific Registry: hereditary angioedema demographics, disease severity, and comorbidities. Ann Allergy Asthma Immunol. 2023;131:766–774.e8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
