

Impact of preoperative intraocular pressure on corneal endothelial cell loss after phacoemulsification in acute primary angle-closure glaucoma with cataracts
- PMID: 40276739
- PMCID: PMC12018442
- DOI: 10.3389/fmed.2025.1533950
Impact of preoperative intraocular pressure on corneal endothelial cell loss after phacoemulsification in acute primary angle-closure glaucoma with cataracts
Abstract
Purpose: This study aimed to assess corneal endothelial cell loss (ECL) following phacoemulsification and intraocular lens implantation (Phaco+IOL) in eyes with acute primary angle-closure glaucoma (APACG) and cataracts under different preoperative intraocular pressure (IOP) levels.
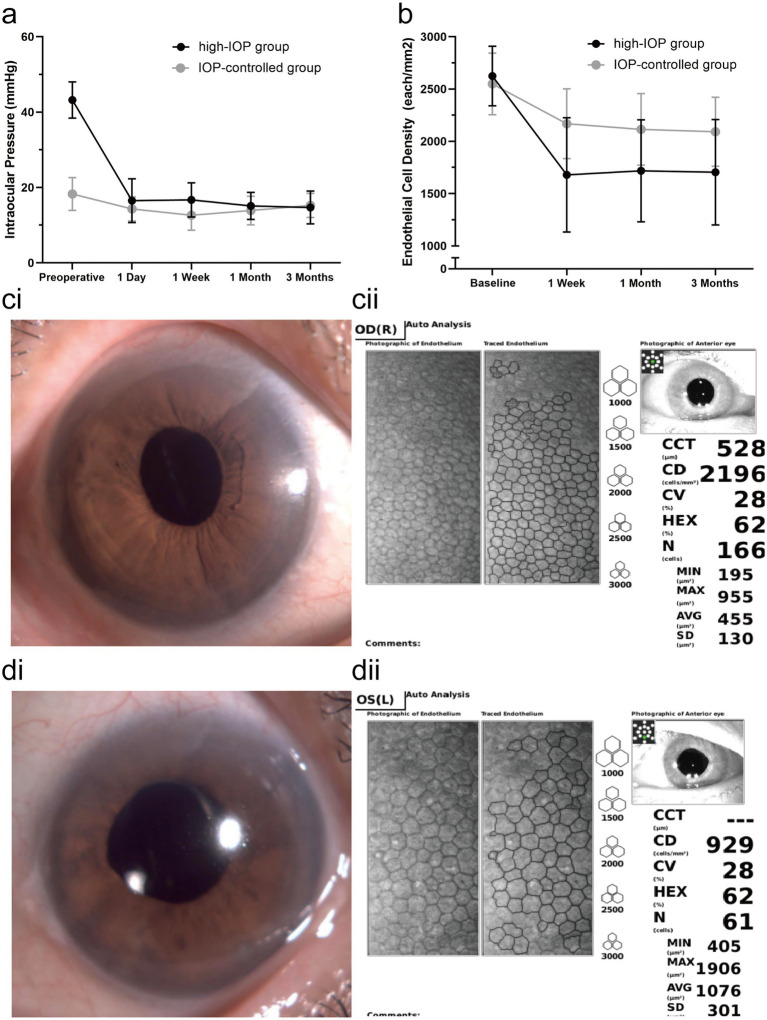
Methods: This non-randomized controlled trial included 75 eyes from 75 patients with APACG and cataracts who underwent Phaco+IOL. All patients received pharmacotherapy and anterior chamber paracentesis before surgery and were grouped according to their preoperative IOP: the high-IOP group (IOP ≥ 25 mmHg) and the IOP-controlled group (IOP < 25 mmHg). IOP, visual outcome, endothelial cell density (ECD), hexagonality (HEX), coefficient of variation (CV), and central corneal thickness (CCT) were evaluated up to 3 months postoperatively. Baseline ECD, HEX, and CV parameters were measured in the contralateral eyes of all patients as a reference and compared with the postoperative results.
Results: The average IOP decreased from 43.2 ± 4.8 mmHg to 16.5 ± 5.8 mmHg (p < 0.001) in the high-IOP group and from 18.3 ± 4.3 mmHg to 14.3 ± 3.2 mmHg (p < 0.001) in the IOP-controlled group on the first postoperative day. The changes in IOP were more significant in the high-IOP group (p < 0.001). The ECD at 3 months was 1705.2 ± 503.8 cells/mm2 in the high-IOP group and 2091.8 ± 330.1 cells/mm2 in the IOP-controlled group (p < 0.001). The ECL rates at 3 months were 35.0% (high-IOP group) and 17.4% (IOP-controlled group) (p < 0.001). The postoperative changes in HEX and CV at 3 months were more significant in the high-IOP group (p < 0.001; p = 0.003). Both groups produced comparable improvements in visual acuity and IOP.
Conclusion: Uncontrolled high IOP (≥ 25 mmHg) before Phaco+IOL in patients with APACG and cataracts is associated with a higher rate of ECL. The rapid and substantial reduction of IOP during surgery may exacerbate corneal endothelial cell loss.
Clinical trial registration: ClinicalTrails.gov, identifier ChiCTR2100052096.
Keywords: acute primary angle-closure glaucoma; corneal endothelial cell loss; endothelial cell density; ocular hypertension; phacoemulsification.
Copyright © 2025 Shen, Liu, Lin, Shao, Niu, Qu, Niu, Zhou, Zhang and Bi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Husain R, Do T, Lai J, Kitnarong N, Nongpiur ME, Perera SA, et al. . Efficacy of phacoemulsification alone vs phacoemulsification with goniosynechialysis in patients with primary angle-closure disease: a randomized clinical trial. JAMA Ophthalmol. (2019) 137:1107–13. doi: 10.1001/jamaophthalmol.2019.2493, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources