

Heterozygous Men1(+/T) Knockout Mice Do Not Develop Bronchopulmonary Neuroendocrine Hyperplasia or Neoplasia but Bronchial Adenocarcinoma
- PMID: 40277511
- PMCID: PMC12024158
- DOI: 10.3390/arm93020007
Heterozygous Men1(+/T) Knockout Mice Do Not Develop Bronchopulmonary Neuroendocrine Hyperplasia or Neoplasia but Bronchial Adenocarcinoma
Abstract
Introduction: Bronchopulmonary Neuroendocrine Neoplasms (NEN) occur in 2-7% of patients with multiple endocrine neoplasia type 1 (MEN1). Precursor lesions have been identified for MEN1-related pancreatic, duodenal, and gastric NEN. The aim of the current study using a MEN1 mouse model was to define the precursor lesions of bronchopulmonary NEN and evaluate the potential prophylactic antitumor effects of somatostatin analogues in a transgenic MEN1 mouse model.
Methods: Fifteen mice, germline heterozygous for Men1(+/T), were treated with subcutaneous injections of lanreotide autogel (Somatuline Autogel®, IPSEN Pharma), while 15 mice were treated with subcutaneous injections of physiologic sodium chloride as the control group. Five mice from each group were euthanized after 12, 15, and 18 months, respectively. The complete lungs were resected and evaluated after hematoxylin and eosin staining and immunohistochemistry for synaptophysin and chromogranin A.
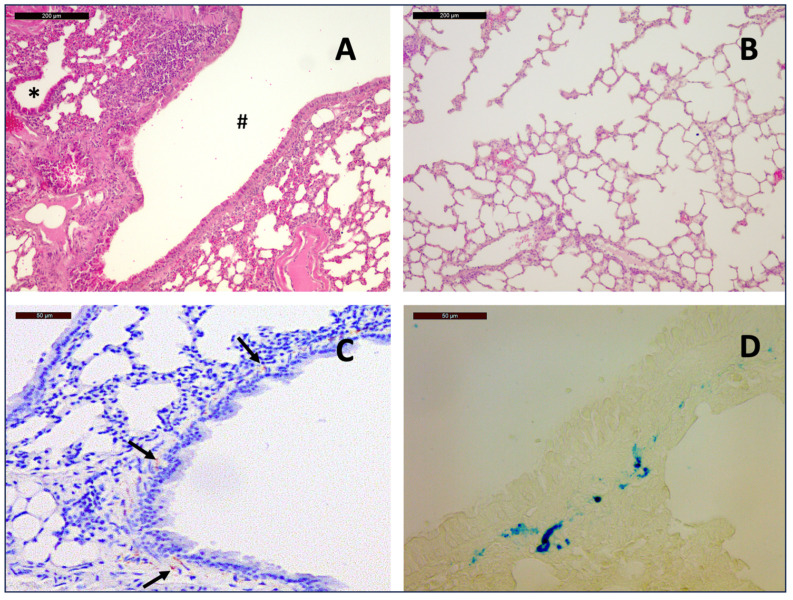
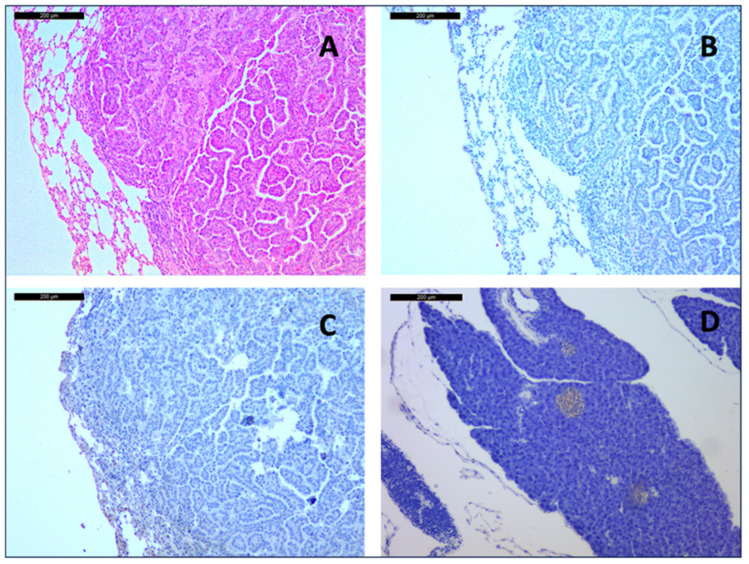
Results: In the lungs of the 30 evaluated mice, whether treated or placebo treated, no bronchopulmonary neuroendocrine cell hyperplasia nor neuroendocrine neoplasia was detected through histopathology. However, pulmonary adenocarcinoma developed in 2 (13%) of the 15 untreated mice and in 1 (7%) of the 15 lanreotide-treated mice.
Conclusions: Heterozygous Men1(+/T) knockout mice do not develop bronchopulmonary NEN or precursor lesions, but pulmonary adenocarcinoma. This surprising result needs to be investigated in more detail.
Keywords: MEN1; bronchial adenocarcinoma; bronchial neuroendocrine neoplasia; multiple endocrine neoplasia.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Chemoprevention with Somatuline© Delays the Progression of Pancreatic Neuroendocrine Neoplasms in a Mouse Model of Multiple Endocrine Neoplasia Type 1 (MEN1).World J Surg. 2019 Mar;43(3):831-838. doi: 10.1007/s00268-018-4839-8. World J Surg. 2019. PMID: 30600364
-
Lanreotide Therapy vs Active Surveillance in MEN1-Related Pancreatic Neuroendocrine Tumors < 2 Centimeters.J Clin Endocrinol Metab. 2020 Jan 1;105(1):dgz007. doi: 10.1210/clinem/dgz007. J Clin Endocrinol Metab. 2020. PMID: 31586182
-
Bronchopulmonary Neuroendocrine Neoplasms and Their Precursor Lesions in Multiple Endocrine Neoplasia Type 1.Neuroendocrinology. 2016;103(3-4):240-7. doi: 10.1159/000435921. Epub 2015 Jun 18. Neuroendocrinology. 2016. PMID: 26113081
-
Progress report on multiple endocrine neoplasia type 1.Fam Cancer. 2025 Jan 18;24(1):15. doi: 10.1007/s10689-025-00440-4. Fam Cancer. 2025. PMID: 39826015 Free PMC article. Review.
-
Pancreatic Neuroendocrine Neoplasms in Multiple Endocrine Neoplasia Type 1.Int J Mol Sci. 2021 Apr 14;22(8):4041. doi: 10.3390/ijms22084041. Int J Mol Sci. 2021. PMID: 33919851 Free PMC article. Review.
References
-
- Chandrasekharappa S.C., Guru S.C., Manickam P., Olufemi S.E., Collins F.S., Emmert-Buck M.R., Debelenko L.V., Zhuang Z., Lubensky I.A., Liotta L.A., et al. Positional cloning of the gene for multiple endocrine neoplasia-type 1. Science. 1997;276:404–407. doi: 10.1126/science.276.5311.404. - DOI - PubMed
-
- Bartsch D.K., Albers M.B., Lopez C.L., Apitzsch J.C., Walthers E.M., Fink L., Fendrich V., Slater E.P., Waldmann J., Anlauf M. Bronchopulmonary Neuroendocrine Neoplasms and Their Precursor Lesions in Multiple Endocrine Neoplasia Type 1. Neuroendocrinology. 2016;103:240–247. doi: 10.1159/000435921. - DOI - PubMed
-
- Goudet P., Murat A., Binquet C., Cardot-Bauters C., Costa A., Ruszniewski P., Niccoli P., Ménégaux F., Chabrier G., Borson-Chazot F., et al. Risk factors and causes of death in MEN1 disease. A GTE (Groupe d’Etude des Tumeurs Endocrines) cohort study among 758 patients. World J. Surg. 2010;34:249–255. doi: 10.1007/s00268-009-0290-1. - DOI - PubMed
-
- Thakker R.V., Newey P.J., Walls G.V., Bilezikian J., Dralle H., Ebeling P.R., Melmed S., Sakurai A., Tonelli F., Brandi M.L. Endocrine Society. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1) J. Clin. Endocrinol. Metab. 2012;97:2990–3011. doi: 10.1210/jc.2012-1230. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
