

Postmastectomy Breast Reconstruction in Patients with Non-Metastatic Breast Cancer: A Systematic Review
- PMID: 40277787
- PMCID: PMC12025830
- DOI: 10.3390/curroncol32040231
Postmastectomy Breast Reconstruction in Patients with Non-Metastatic Breast Cancer: A Systematic Review
Abstract
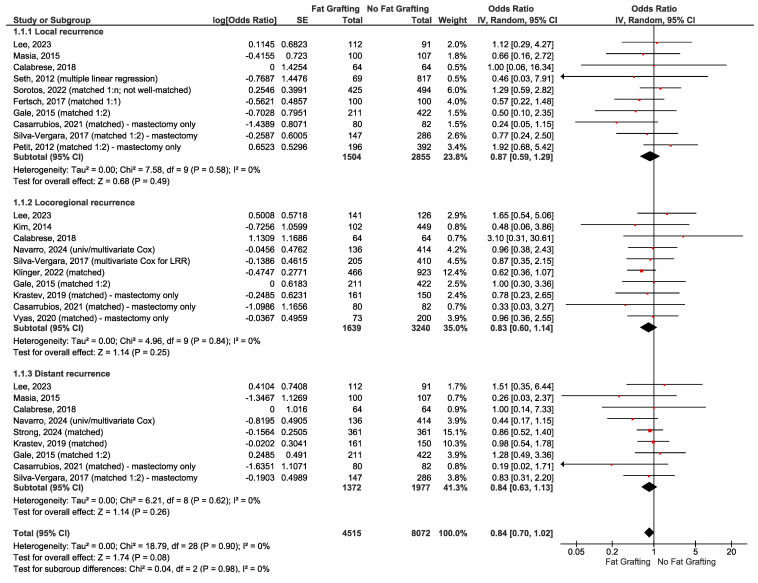
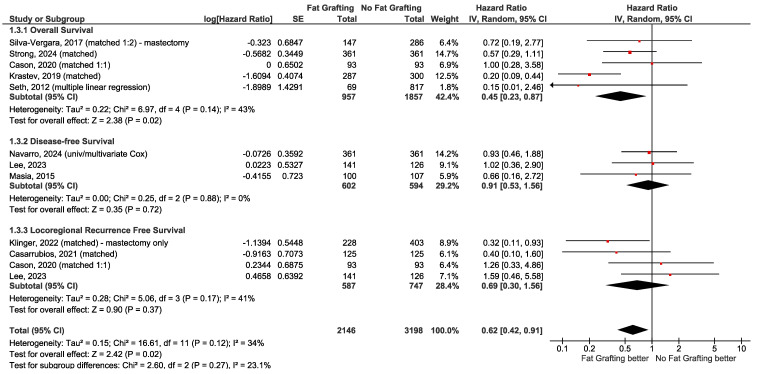
Breast reconstruction after mastectomy improves the quality of life for many patients with breast cancer. There is uncertainty regarding eligibility criteria for reconstruction, timing (immediate or delayed-with or without radiotherapy), outcomes of nipple-sparing compared to skin-sparing mastectomy, selection criteria and surgical factors influencing outcomes of nipple-sparing mastectomy, prepectoral versus subpectoral implants, use of acellular dermal matrix, and use of autologous fat grafting. We conducted a systematic review of these topics to be used as the evidence base for an updated clinical practice guideline on breast reconstruction for Ontario Health (Cancer Care Ontario). The protocol was registered on PROSPERO, CRD42023409083. Medline, Embase, and Cochrane databases were searched until August 2024, and 229 primary studies met the inclusion criteria. Most studies were retrospective non-randomized comparative studies; 5 randomized controlled trials were included. Results suggest nipple-sparing mastectomy is oncologically safe, provided there is no clinical, radiological, or pathological indication of nipple-areolar complex involvement. Surgical factors, including incision location, may affect rates of complications such as necrosis. Both immediate and delayed reconstruction have similar long-term outcomes; however, immediate reconstruction may result in better short to medium-term quality of life. Evidence on whether radiotherapy should modify the timing of initial reconstruction or expander-implant exchange was very limited; studies delayed reconstruction after radiotherapy by at least 3 months and, more commonly, at least 6 months to avoid the period of acute radiation injury. Radiation after immediate reconstruction is a reasonable option. Surgical complications are similar between prepectoral and dual-plane or subpectoral reconstruction; prepectoral placement may give a better quality of life due to lower rates of long-term complications such as pain and animation deformity. Autologous fat grafting was found to be oncologically safe; its use may improve quality of life and aesthetic results.
Keywords: acellular dermal matrix; autologous fat grafting; autologous reconstruction; breast implants; breast reconstruction; delayed reconstruction; immediate reconstruction; nipple-sparing mastectomy; prepectoral; subpectoral.
Conflict of interest statement
C.S. reported receiving honoraria for chairing or moderating two speaker series on updates in oncological advancements to regional surgical, medical, and radiation oncologists. F.C.W. was the surgical oncology provincial lead, a program of Ontario Health (Cancer Care Ontario). The other authors declare no conflicts of interest. The funder approved the research questions and project plan prior to the commencement of the systematic review. The sponsor had no role in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Postmastectomy Breast Reconstruction in Patients with Non-Metastatic Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline.Curr Oncol. 2025 Jun 17;32(6):357. doi: 10.3390/curroncol32060357. Curr Oncol. 2025. PMID: 40558300 Free PMC article.
-
Implants versus autologous tissue flaps for breast reconstruction following mastectomy.Cochrane Database Syst Rev. 2024 Oct 31;10(10):CD013821. doi: 10.1002/14651858.CD013821.pub2. Cochrane Database Syst Rev. 2024. PMID: 39479986
-
Skin-sparing mastectomy for the treatment of breast cancer.Cochrane Database Syst Rev. 2023 Mar 27;3(3):CD010993. doi: 10.1002/14651858.CD010993.pub2. Cochrane Database Syst Rev. 2023. PMID: 36972145 Free PMC article.
-
Different types of implants for reconstructive breast surgery.Cochrane Database Syst Rev. 2016 May 16;2016(5):CD010895. doi: 10.1002/14651858.CD010895.pub2. Cochrane Database Syst Rev. 2016. PMID: 27182693 Free PMC article.
-
Oncoplastic breast-conserving surgery for women with primary breast cancer.Cochrane Database Syst Rev. 2021 Oct 29;10(10):CD013658. doi: 10.1002/14651858.CD013658.pub2. Cochrane Database Syst Rev. 2021. PMID: 34713449 Free PMC article.
Cited by
-
Postmastectomy Breast Reconstruction in Patients with Non-Metastatic Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline.Curr Oncol. 2025 Jun 17;32(6):357. doi: 10.3390/curroncol32060357. Curr Oncol. 2025. PMID: 40558300 Free PMC article.
References
-
- Winters Z.E., Benson J.R., Pusic A.L. A systematic review of the clinical evidence to guide treatment recommendations in breast reconstruction based on patient-reported outcome measures and health-related quality of life. Ann. Surg. 2010;252:929–942. doi: 10.1097/SLA.0b013e3181e623db. - DOI - PubMed
-
- Pusic A.L., Klassen A.F., Snell L., Cano S.J., McCarthy C., Scott A., Cemal Y., Rubin L.R., Cordeiro P.G. Measuring and managing patient expectations for breast reconstruction: Impact on quality of life and patient satisfaction. Expert Rev. Pharmacoecon. Outcomes Res. 2012;12:149–158. doi: 10.1586/erp.11.105. - DOI - PMC - PubMed
-
- Kronowitz S.J. A systematic review of the clinical evidence to guide treatment recommendations in breast reconstruction based on patient-reported outcome measures and health-related quality of life: Winters ZE, Benson JR, Pusic AL (Univ of Bristol, UK; Univ of Cambridge, UK; Memorial Sloan-Kettering Cancer Ctr, NY) Ann Surg 252:929-942, 2010. Breast Dis. 2011;22:420–422. doi: 10.1016/j.breastdis.2011.10.042. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
