

The Prediction of Intrapartum Fetal Compromise According to the Expected Fetal Weight
- PMID: 40278319
- PMCID: PMC12028832
- DOI: 10.3390/jpm15040140
The Prediction of Intrapartum Fetal Compromise According to the Expected Fetal Weight
Abstract
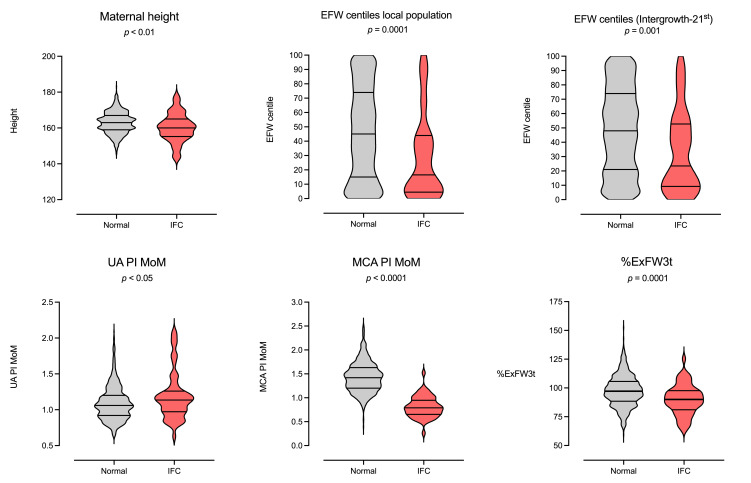
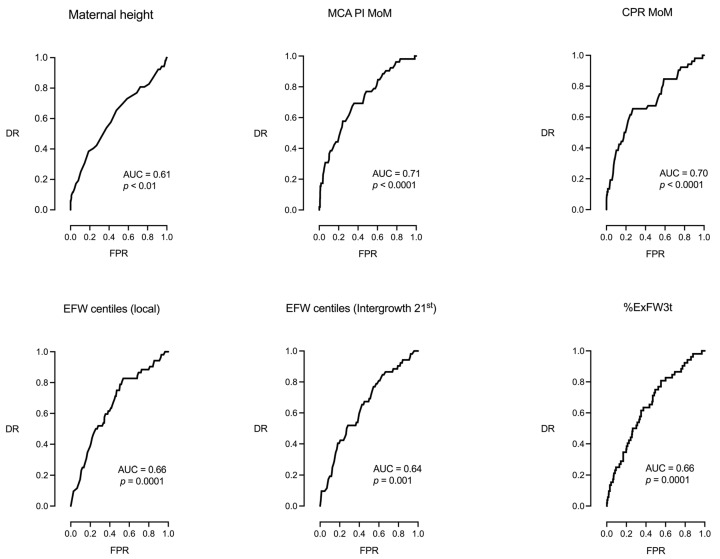
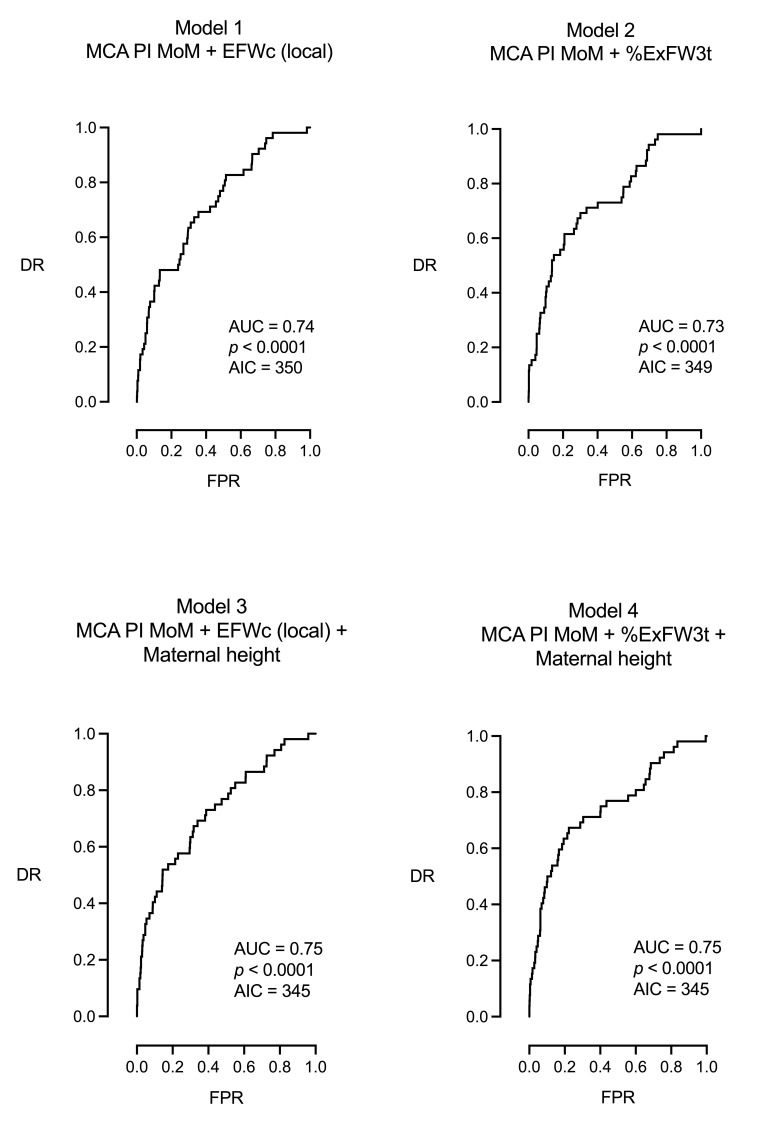
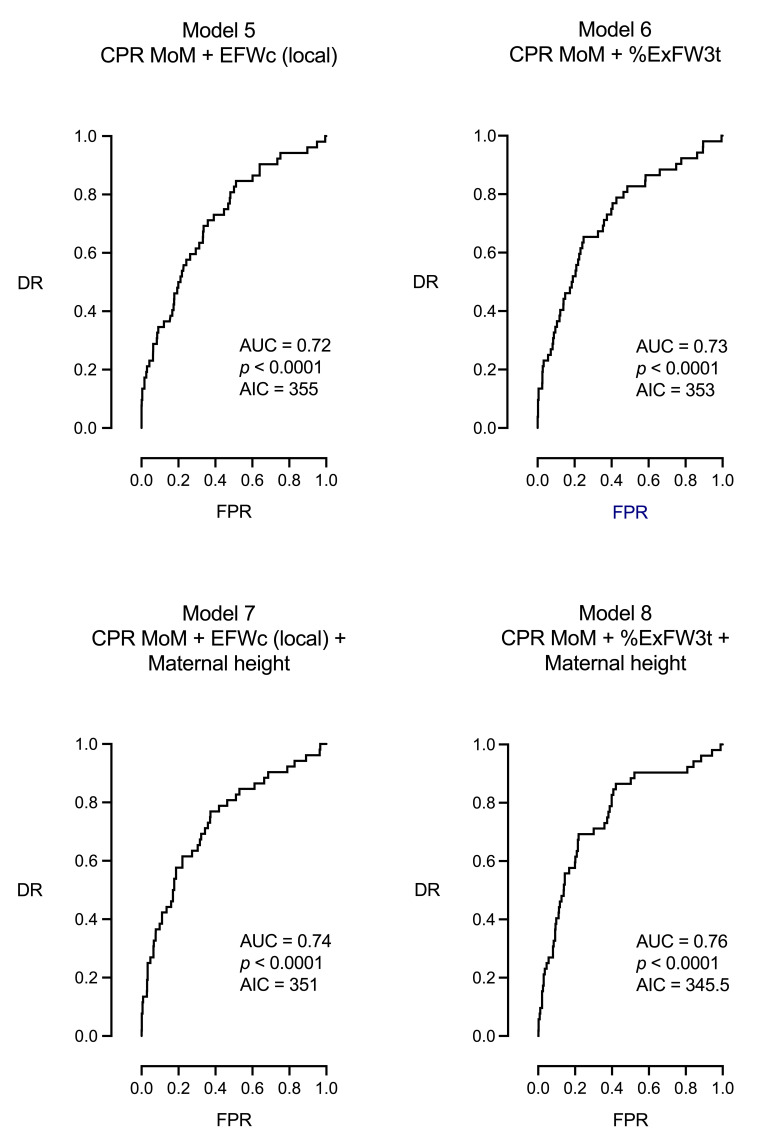
Objectives: To assess the predictive accuracy of the expected fetal weight in the third trimester (ExFW3t), based on the estimated fetal weight (EFW) at mid-trimester ultrasound scan, for the prediction of intrapartum fetal compromise (IFC) (an abnormal intrapartum fetal heart rate or intrapartum fetal scalp pH requiring urgent cesarean section). Methods: This retrospective study included 777 singleton pregnancies that underwent a 20-week study and a 3t scan. The extrapolated EFW at 20 weeks to the 3t or ExFW3t was considered a proxy of the potential growth. The percentage difference with the actual 3t EFW (%ExFW3t) was compared with other ultrasonographic and clinical parameters-EFW centile (EFWc), middle cerebral artery pulsatility index (MCA PI) in multiples of the median (MoM), umbilical artery (UA) PI MoM, cerebroplacental ratio (CPR) MoM, and maternal height-for the prediction of IFC by means of the area under the curve (AUC) and Akaike Information Criteria (AIC). Results: Pregnancies with IFC presented higher values of UA PI MoM (1.19 vs. 1.09, p = 0.0460) and lower values of population and Intergrowth EFWc (45.9 vs. 28.9, p < 0.0001, 48.4 vs. 33.6, p = 0.0004), MCA PI MoM (0.97 vs. 0.81, p < 0.0001), CPR MoM (1.01 vs. 0.79, p < 0.0001), %ExFW3t (89.9% vs. 97.5%, p = 0.0003), and maternal height (160.2 vs. 162.9, p = 0.0083). Univariable analysis selected maternal height, EFWc, %ExFW3t, and UA PI MoM as significant parameters. However, %ExFW3t did not surpass the prediction ability of cerebral Doppler. Finally, multivariable analysis showed that the best models for the prediction of IFC resulted from the combination of cerebral Doppler (MCA PI MoM or CPR MoM), fetal weight (%ExFW3t or EFWc), and maternal height (AUC 0.75/0.76, AIC 345, p < 0.0001). Conclusions: Fetal weight-related parameters, including %ExFW3t, a proxy of the proportion of potential growth achieved in the 3t, were less effective than fetal cerebral Doppler for the prediction of IFC. The best performance was achieved by combining hemodynamic, ponderal, and clinical data.
Keywords: cerebroplacental ratio; estimated fetal weight; fetal growth restriction; genetic growth potential; intrapartum fetal compromise; middle cerebral artery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Cerebroplacental Ratio Prediction of Intrapartum Fetal Compromise according to the Interval to Delivery.Fetal Diagn Ther. 2022;49(4):196-205. doi: 10.1159/000525162. Epub 2022 Jun 7. Fetal Diagn Ther. 2022. PMID: 35671735
-
The fetal cerebral Doppler in the last weeks of pregnancy can select very small fetuses unlikely to present intrapartum compromise.J Matern Fetal Neonatal Med. 2025 Dec;38(1):2456989. doi: 10.1080/14767058.2025.2456989. Epub 2025 Jan 26. J Matern Fetal Neonatal Med. 2025. PMID: 39864846
-
Prediction of adverse perinatal outcome by cerebroplacental ratio adjusted for estimated fetal weight.Ultrasound Obstet Gynecol. 2018 Mar;51(3):381-386. doi: 10.1002/uog.17458. Epub 2018 Feb 7. Ultrasound Obstet Gynecol. 2018. PMID: 28294442
-
Management of fetuses with apparent normal growth and abnormal cerebroplacental ratio: A risk-based approach near term.Acta Obstet Gynecol Scand. 2024 Feb;103(2):334-341. doi: 10.1111/aogs.14732. Epub 2023 Dec 4. Acta Obstet Gynecol Scand. 2024. PMID: 38050342 Free PMC article.
-
Prediction of Cesarean Section for Intrapartum Fetal Compromise: A Multivariable Model from a Prospective Observational Approach.J Pers Med. 2024 Jun 20;14(6):658. doi: 10.3390/jpm14060658. J Pers Med. 2024. PMID: 38929879 Free PMC article.
Cited by
-
Predicting Fetal Growth with Curve Fitting and Machine Learning.Bioengineering (Basel). 2025 Jul 3;12(7):730. doi: 10.3390/bioengineering12070730. Bioengineering (Basel). 2025. PMID: 40722422 Free PMC article.
References
-
- Smith-Bindman R., Chu P.W., Ecker J., Feldstein V.A., Filly R.A., Bacchetti P. Adverse birth outcomes in relation to prenatal sonographic measurements of fetal size. J. Ultrasound Med. 2003;22:347–356; quiz 357–358. - PubMed
-
- Morales-Roselló J., Cañada Martínez A.J., Scarinci E., Perales Marín A. Comparison of Cerebroplacental Ratio, Intergrowth-21st Standards, Customized Growth, and Local Population References for the Prediction of Fetal Compromise: Which Is the Best Approach? Fetal Diagn. Ther. 2019;46:341–352. - PubMed
-
- Morales-Roselló J., Martinez-Gonzalez L., Santonja-Lucas J.J. Predicted and actual fetal weight throughout the last trimester. J. Ultrasound Med. 1997;16:711–717. - PubMed
-
- Figueras F., Meler E., Iraola A., Eixarch E., Coll O., Figueras J., Francis A., Gratacos E., Gardosi J. Customized birthweight standards for a Spanish population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008;136:20–24. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
