

Comparing venous wall effects using the empty vein ablation technique with VELEX catheter, endovenous laser ablation and foam sclerotherapy in an animal model
- PMID: 40280361
- PMCID: PMC12149593
- DOI: 10.1016/j.jvsv.2025.102251
Comparing venous wall effects using the empty vein ablation technique with VELEX catheter, endovenous laser ablation and foam sclerotherapy in an animal model
Abstract
Objective: To describe residual intima and the average media thickness persisted after the empty vein ablation (EVA) technique, endovenous laser ablation (EVLA), and foam sclerotherapy (FS) in a sheep in vivo model.
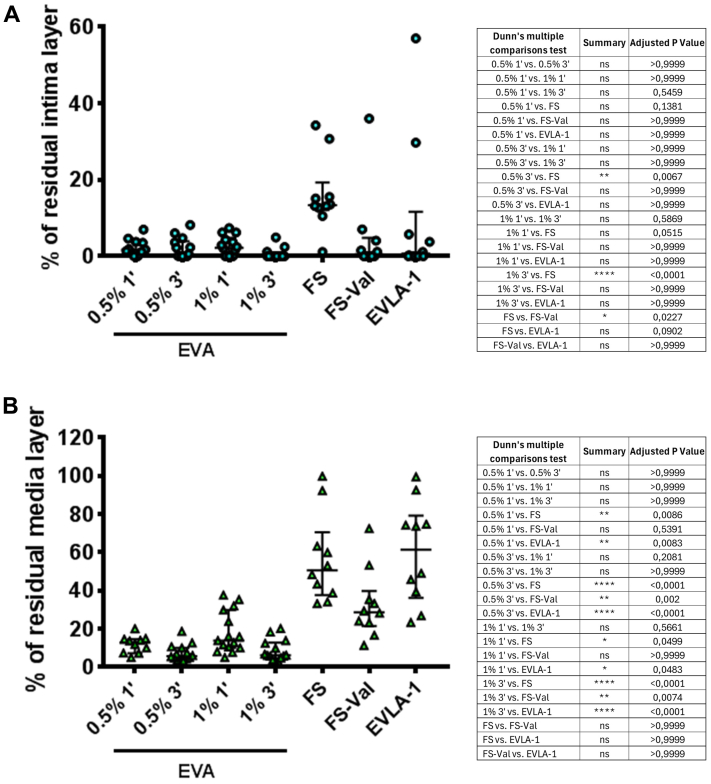
Methods: Six iliofemoral and two jugular sheep vein axes were treated as follows: four with EVA (using polidocanol [POL] 0.5% or 1% with 1 or 3 minutes as contact time), two with FS (FS-1 and FS during Valsalva maneuver [FS-Val], POL1% for 10 minutes), and two with EVLA (1470 nm radial, 80 J/cm2).
Results: The average percentage of residual intima layer was 2% (interquartile range [IQR]: 1%-4%) for EVA-POL0.5%-1 minute, 1% (IQR: 0%-3.5%) for EVA-POL0.5%-3 minutes, 2% (IQR: 0%-4%) for EVA-POL1%-1 minute, 0 for EVA-POL1%-3 minutes, 13% (IQR: 13%-15.7%) for FS, 1% (IQR: 0%-3%) for FS-Val, and 1% (IQR: 0%-6%) for EVLA. The average percentage of residual media thickness was 13% (IQR: 8%-15%) for EVA-POL0.5%-1 minute, 6% (IQR: 4%-9%) for EVA-POL0.5%-3 minutes, 13% (IQR: 10%-27%) for EVA-POL1%-1 minute, 6% (IQR: 5%-12%) for EVA-POL1%-3 minutes, 51% (IQR: 40%-62%) for FS, 29% (IQR: 23%-35%) for FS-Val, and 62% (IQR: 41%-75%) for EVLA.
Conclusions: EVA demonstrated better results in vein wall damage compared with EVLA and FS, both in intima and media layers.
Clinical relevance: This study provides crucial insights into the effectiveness of different vein treatment techniques, particularly the empty vein ablation method, in minimizing residual intima and media thickness. By evaluating these outcomes in a sheep model, it highlights how empty vein ablation may lead to more vein wall damage compared with endovenous laser ablation and foam sclerotherapy. For clinicians, understanding the comparative efficacy of these treatments is vital for optimizing patient care in managing venous diseases. As the field evolves, these findings could influence clinical decision-making, encouraging the adoption of techniques that promote better long-term outcomes for patients.
Keywords: Chronic venous disease; Empty vein ablation; Sclerotherapy; Varicose veins.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures M.S. is inventor of empty vein ablation technology and the founder, CMO, and board member of I-VASC S.r.l., which is developing the VELEX device for commercial uses. The remaining authors report no conflicts.
Figures





References
-
- De Maeseneer M.G., Kakkos S.K., Aherne T., et al. Editor's choice - European Society for Vascular Surgery (ESVS) 2022 clinical practice guidelines on the management of chronic venous disease of the lower limbs. Eur J Vasc Endovasc Surg. 2022;63:184–267. - PubMed
-
- Hamel-Desnos C., Allaert F.A. Liquid versus foam sclerotherapy. Phlebology. 2009;24:240–246. - PubMed
-
- Salerno M., Bissacco D., Chi Y.W., Narayanan S., Addis A., Dellavia C. Empty vein ablation innovative technique for chronic venous disease treatment: proof of concept and ex-vivo analysis. Int Angiol. 2023;42:420–426. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
