

Intratumoral microbiota predicts the response to neoadjuvant chemoimmunotherapy in triple-negative breast cancer
- PMID: 40280564
- PMCID: PMC12035477
- DOI: 10.1136/jitc-2024-010365
Intratumoral microbiota predicts the response to neoadjuvant chemoimmunotherapy in triple-negative breast cancer
Abstract
Background: Neoadjuvant immunotherapy combined with chemotherapy (Chemo-IM) is associated with significantly improved pathological complete response (pCR) rates and long-term survival outcomes in patient with early-stage triple-negative breast cancer (TNBC). However, only a small proportion of patients benefit from the addition of immunotherapy. Here, we explored and confirmed the role of intratumoral microbiota in screening patients with TNBC who are likely to benefit from neoadjuvant Chemo-IM.
Methods: Patients with previously untreated, non-metastatic TNBC receiving neoadjuvant Chemo-IM were enrolled. Differences in the intratumoral microbiota between the pCR and non-pCR groups were explored via 16S rDNA sequencing (16S-seq). Single-cell transcriptome sequencing (scRNA-seq) was employed to profile the tumor microenvironment (TME). Moreover, correlations between the intratumor microbiota and the TME were explored. Finally, machine-learning models based on the intratumoral microbiota were constructed to predict pCR.
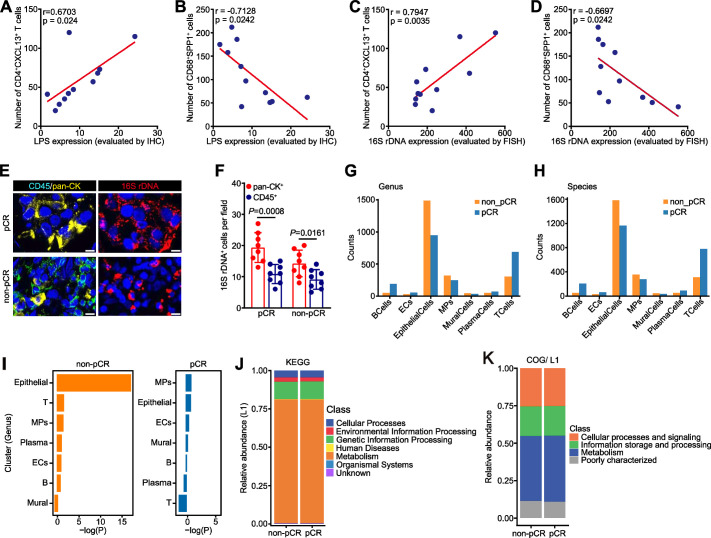
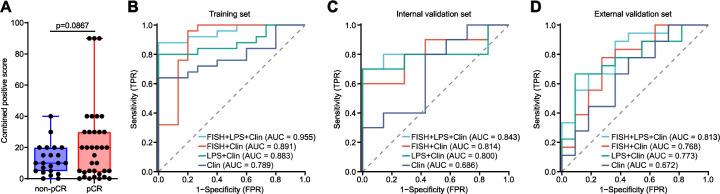
Results: A total of 89 female patients with early-stage TNBC treated by neoadjuvant Chemo-IM were enrolled. We found that the pCR group had greater diversity and a higher load of intratumoral microbiota than the non-pCR group. Intriguingly, scRNA-seq revealed significantly increased T cell infiltration and decreased tumor-associated macrophage infiltration into tumors in the pCR group. Moreover, intratumoral microbiota load was positively associated with CD4+CXCL13+ T cell infiltration and negatively associated with CD68+SPP1+ macrophage infiltration. Combined analysis of 16S-seq and scRNA-seq data revealed that intratumoral microbiota were present in both cancer and immune cells. Finally, we developed a model incorporating intratumoral microbiota and clinicopathological characteristics, and it showed strong power for predicting pCR to neoadjuvant Chemo-IM.
Conclusions: Intratumoral microbiota may serve as a strong and specific predictor of the response of patients with early-stage TNBC to neoadjuvant Chemo-IM. Our findings could contribute to the development of individualized Chemo-IM strategies for treating TNBC.
Keywords: Biomarker; Breast Cancer; Immunotherapy; Intratumoral.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: No, there are no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous