

Non-aggressive, sinus-type greater sphenoid wing dural arteriovenous fistula with shunt point in the laterocavernous sinus mimicking a cavernous sinus dural arteriovenous fistula converted to aggressive, non-sinus-type
- PMID: 40280581
- PMCID: PMC12034921
- DOI: 10.1136/bcr-2025-265715
Non-aggressive, sinus-type greater sphenoid wing dural arteriovenous fistula with shunt point in the laterocavernous sinus mimicking a cavernous sinus dural arteriovenous fistula converted to aggressive, non-sinus-type
Abstract
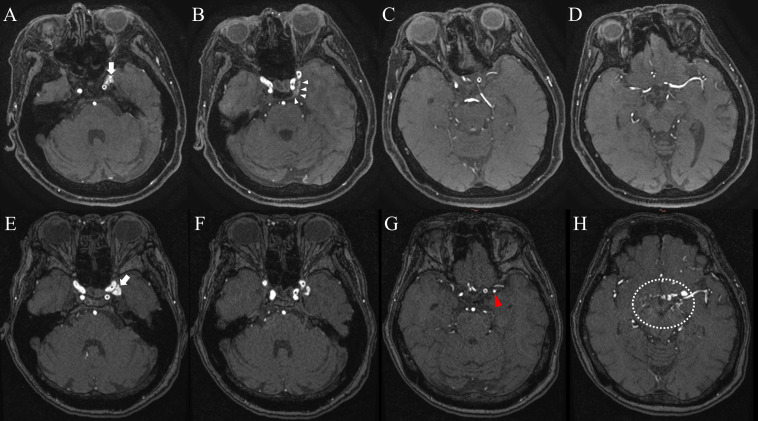
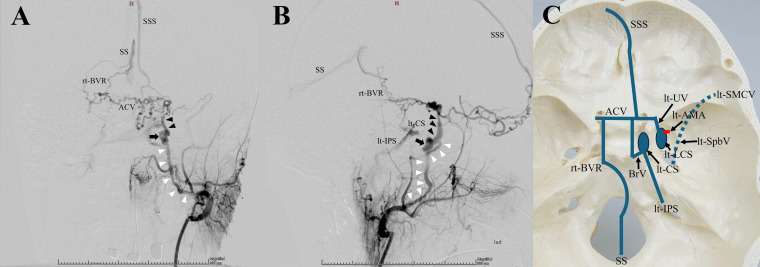
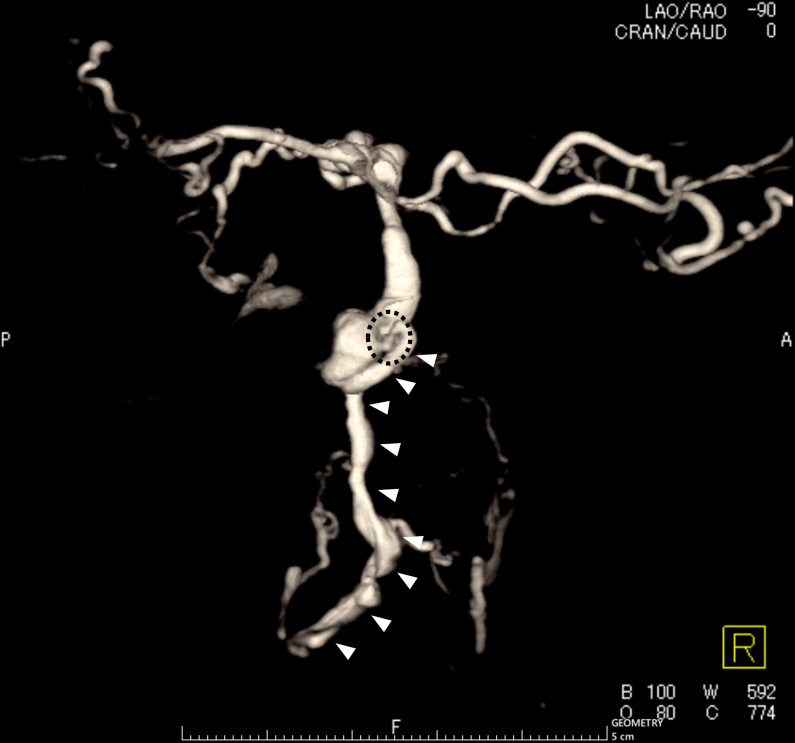
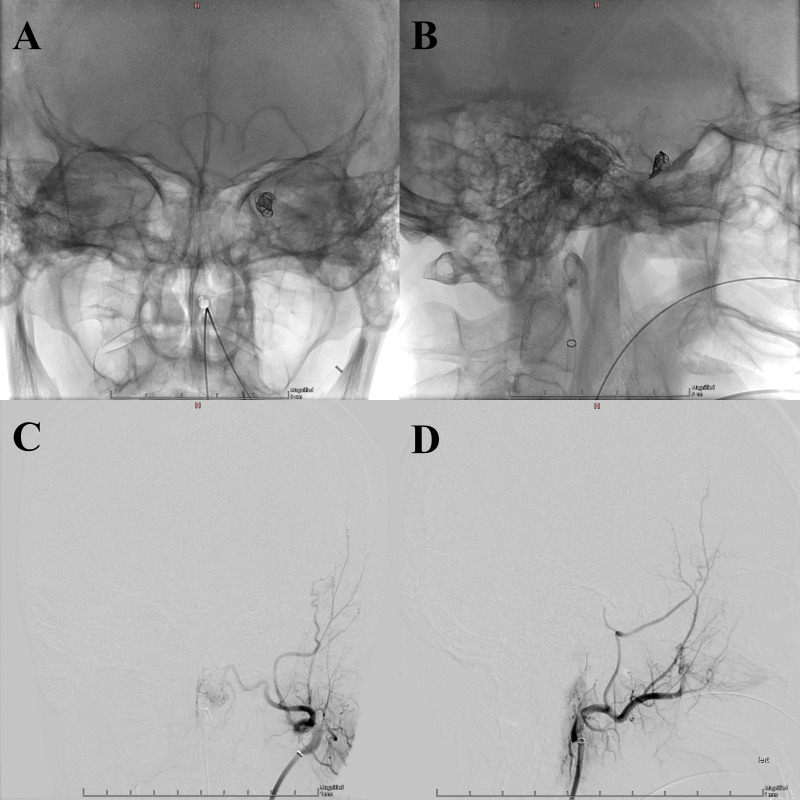
Sphenoid wing dural arteriovenous fistulae (DAVFs) are rare. Although the imaging findings of greater sphenoid wing DAVFs may resemble those of cavernous sinus DAVFs (CSDAVFs), their respective presentations differ. Benign CSDAVFs rarely convert to the aggressive type. Conversely, as greater sphenoid wing DAVFs are often of the aggressive type, with intracranial cortical venous reflux and varices, treatment is recommended. Sphenoid wing DAVFs tend to be of the non-sinus type, and transarterial embolisation is often an effective endovascular treatment. We present a case of an asymptomatic greater sphenoid wing DAVF mimicking a CSDAVF that converted from a non-aggressive sinus-type to an aggressive non-sinus-type due to compartmentalisation and thrombotic occlusion. Transarterial embolisation with Onyx and a transarterial venous coil resulted in complete disappearance of the DAVF. Greater sphenoid wing DAVFs can be misdiagnosed as CSDAVFs and require accurate imaging evaluation and careful follow-up, even in asymptomatic or non-aggressive cases.
Keywords: Neuroimaging; Stroke.
© BMJ Publishing Group Limited 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Aggressive cavernous sinus dural arteriovenous fistula: Angioarchitecture analysis and embolization by various approaches.J Chin Med Assoc. 2016 Mar;79(3):152-8. doi: 10.1016/j.jcma.2015.09.001. Epub 2016 Jan 29. J Chin Med Assoc. 2016. PMID: 26830630
-
Intra-arterial onyx embolisation of sphenobasilar sinus fistula using pressure cooker technique: case report and review of the literature.Neuroradiol J. 2021 Apr;34(2):131-134. doi: 10.1177/1971400920972512. Epub 2020 Nov 11. Neuroradiol J. 2021. PMID: 33176554 Free PMC article. Review.
-
Middle cranial fossa sphenoidal region dural arteriovenous fistulas: anatomic and treatment considerations.AJNR Am J Neuroradiol. 2013 Feb;34(2):373-80. doi: 10.3174/ajnr.A3193. Epub 2012 Jul 12. AJNR Am J Neuroradiol. 2013. PMID: 22790245 Free PMC article.
-
Endovascular treatment of the cavernous sinus dural arteriovenous fistula: current status and considerations.Int J Med Sci. 2020 May 1;17(8):1121-1130. doi: 10.7150/ijms.45210. eCollection 2020. Int J Med Sci. 2020. PMID: 32410842 Free PMC article. Review.
-
Evaluation for shunted pouches of cavernous sinus dural arteriovenous fistula and the treatment outcome of transvenous embolization.Interv Neuroradiol. 2018 Apr;24(2):189-196. doi: 10.1177/1591019917743064. Epub 2017 Nov 29. Interv Neuroradiol. 2018. PMID: 29183173 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources