

Risk factors for in-hospital mortality in surgical patients with abdominal sepsis in China: a nested case-control study
- PMID: 40280608
- PMCID: PMC12035482
- DOI: 10.1136/bmjopen-2024-092310
Risk factors for in-hospital mortality in surgical patients with abdominal sepsis in China: a nested case-control study
Abstract
Objectives: To delineate the clinical characteristics and investigate the determinants that may affect the prognosis of surgical patients with abdominal sepsis.
Design: A case-control study was nested in a cohort of surgical patients with abdominal sepsis between 2008 and 2022. We extracted patient' medical records to execute descriptive statistical analyses. Multiple logistic regression models and subgroup analysis were employed to elucidate the risk factors of in-hospital mortality.
Setting: Two tertiary hospitals in China.
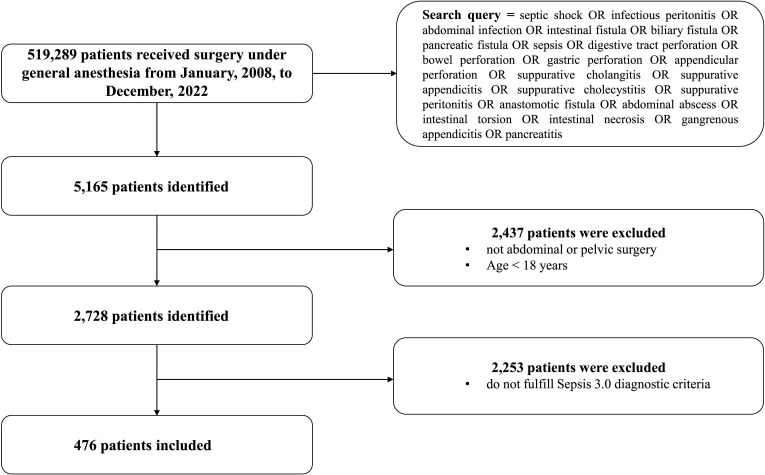
Participants: 476 surgical patients diagnosed with abdominal sepsis between 2008 and 2022 were analysed.
Interventions: None.
Outcome measures: Descriptive statistics were used to examine pertinent patient information, including demographic details, laboratory findings, surgical interventions and anaesthetic records. Multivariate logistic regression was used to identify independent risk factors for in-hospital mortality. Subgroup analyses were conducted to explore the impact of specific clinical characteristics on outcomes.
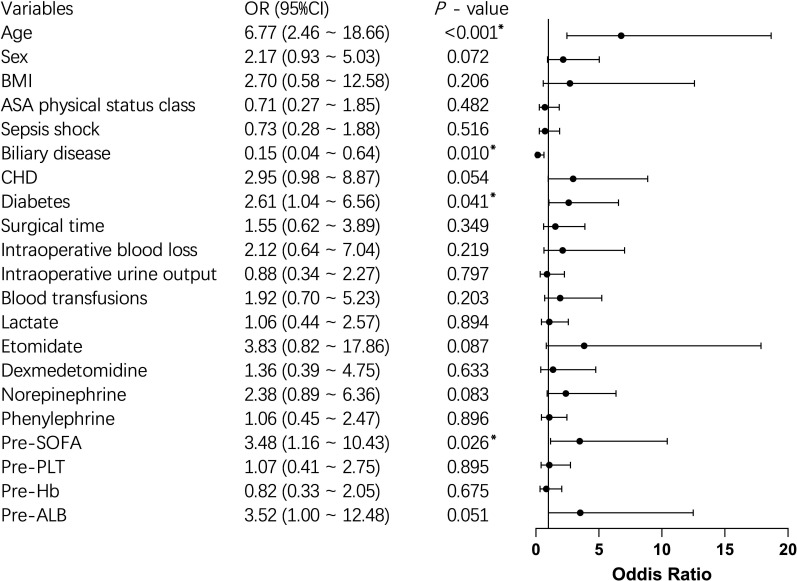
Results: 476 patients diagnosed with abdominal sepsis were analysed, exhibiting an in-hospital mortality rate of 7.56%. Advanced age (OR 6.77, 95% CI 2.46 to 18.66, p<0.001), the presence of diabetes (OR 2.61, 95% CI 1.04 to 6.56, p=0.041) and higher preoperative Sequential Organ Failure Assessment (SOFA) score (OR 3.48, 95% CI 1.16 to 10.43, p=0.026) were identified as significant predictors of increased in-hospital mortality risk through a multinomial logistic regression model. Conversely, individuals afflicted with biliary diseases (OR 0.15, 95% CI 0.04 to 0.64, p=0.010) demonstrated a reduced risk of in-hospital mortality. Subgroup analysis revealed that low serum albumin levels emerged as a risk factor for in-hospital mortality in the patients with gastrointestinal diseases (OR 20.23, 95% CI 2.21 to 184.84, p=0.008) or advanced age (OR 10.52, 95% CI 2.29 to 48.31, p=0.002) through multinomial logistic regression analysis.
Conclusion: In this retrospective analysis, we delineated the clinical characteristics of surgical patients with abdominal sepsis and pinpointed risk factors associated with in-hospital mortality. These findings underscore the necessity for more tailored perioperative management strategies for patients with sepsis characterised by advanced age, diabetes, higher preoperative SOFA score and reduced preoperative albumin levels. Clinicians should prioritise early recognition and aggressive management of these high-risk individuals, including timely surgical intervention, optimisation of nutritional status and vigilant monitoring of organ function. These insights underscore the critical role of individualised care in enhancing the prognosis of surgical patients with abdominal sepsis.
Trial registration number: ChiCTR2400081823.
Keywords: adult anaesthesia; gastrointestinal infections; intensive & critical care; mortality; risk factors; surgery.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
[A multicenter clinical study of critically ill patients with sepsis complicated with acute kidney injury in Beijing: incidence, clinical characteristics and outcomes].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Jun;36(6):567-573. doi: 10.3760/cma.j.cn121430-20240210-00124. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38991953 Chinese.
-
Validation of prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among cardiac-, thoracic-, and vascular-surgery patients admitted to a cardiothoracic intensive care unit.J Card Surg. 2020 Jan;35(1):118-127. doi: 10.1111/jocs.14331. Epub 2019 Nov 11. J Card Surg. 2020. PMID: 31710762
-
Platelet-to-lymphocyte ratio as a prognostic predictor of mortality for sepsis: interaction effect with disease severity-a retrospective study.BMJ Open. 2019 Jan 25;9(1):e022896. doi: 10.1136/bmjopen-2018-022896. BMJ Open. 2019. PMID: 30782690 Free PMC article.
-
Sequential Organ Failure Assessment Component Score Prediction of In-hospital Mortality From Sepsis.J Intensive Care Med. 2020 Aug;35(8):810-817. doi: 10.1177/0885066618795400. Epub 2018 Aug 30. J Intensive Care Med. 2020. PMID: 30165769 Free PMC article.
-
Predictive Value of Serum Albumin Level for the Prognosis of Severe Sepsis Without Exogenous Human Albumin Administration: A Prospective Cohort Study.J Intensive Care Med. 2018 Dec;33(12):687-694. doi: 10.1177/0885066616685300. Epub 2016 Dec 26. J Intensive Care Med. 2018. PMID: 28013574
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical