

Machine learning-based forecasting of daily acute ischemic stroke admissions using weather data
- PMID: 40281217
- PMCID: PMC12032073
- DOI: 10.1038/s41746-025-01619-w
Machine learning-based forecasting of daily acute ischemic stroke admissions using weather data
Abstract
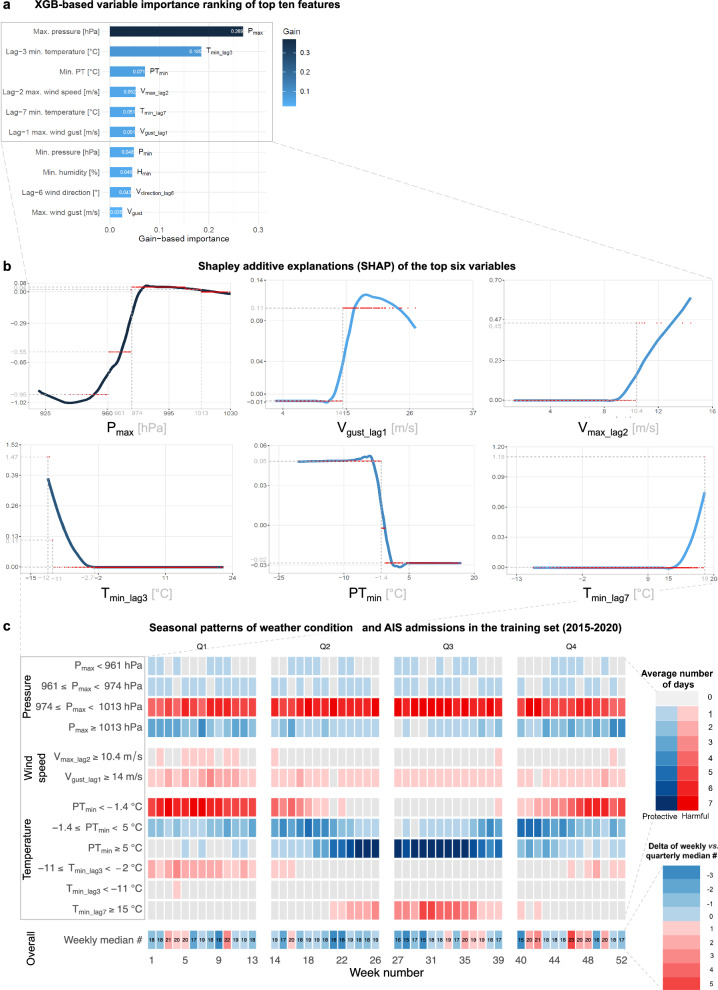
The climate crisis underscores the need for weather-based predictive analytics in healthcare, as weather factors contribute to ~11% of the global stroke burden. Therefore, we developed machine learning models using locoregional weather data to forecast daily acute ischemic stroke (AIS) admissions. An AIS cohort of 7914 patients admitted between 2015 and 2021 at the tertiary University Medical Center Mannheim, Germany, with a 600,000-population catchment area, was geospatially matched to German Weather Service data. Poisson regression, boosted generalized additive models, support vector machines, random forest, and extreme gradient boosting (XGB) were evaluated within a time-stratified nested cross-validation framework. XGB performed best (mean absolute error: 1.21 cases/day). Maximum air pressure was the top predictor, with temperature exhibiting a bimodal link. Cold and heat stressor days (Tmin_lag3 < -2 °C; Tperceived < -1.4 °C; Tmin_lag7 > 15 °C) and stormy conditions (wind gusts > 14 m/s) increased stroke admissions. This generalizable framework could aid real-time hospital planning, effective care and forecasting of various weather-related disease burdens.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: M.E.M. reports unrelated consultancy to EppData GmbH and Siemens Healthineers GmbH, Germany. The remaining authors declare no competing interests. Ethics approval: This single-center retrospective cohort study entitled “Weather-based Stroke Event and Outcome Risk Modeling (WE-STORM)” was approved by the local use- and access- (UAC) and ethics committees (Medical Ethics Commission II, Medical Faculty Mannheim, Heidelberg University, approval nr.: 2022-800R-MA). All methods were carried out following institutional guidelines and regulations. The ethics committee waived written informed consent due to the retrospective nature of the analyses.
Figures


 is located in the state of Baden–Wuerttemberg at (e) the corner of a German tri-state area (Rhineland Palatinate and Hesse; light blue bounding box). UMC is the primary tertiary care provider in Mannheim, the largest city in the region and the second largest in the state, with a population of 310,000 and a catchment area of over 600,000 people between Frankfurt (
is located in the state of Baden–Wuerttemberg at (e) the corner of a German tri-state area (Rhineland Palatinate and Hesse; light blue bounding box). UMC is the primary tertiary care provider in Mannheim, the largest city in the region and the second largest in the state, with a population of 310,000 and a catchment area of over 600,000 people between Frankfurt ( ) and Stuttgart. f Geospatial distribution highlighting the density of ischemic strokes per 100,000 population in the catchment area of UMC using the postal code-based distribution of patients’ home locations. The top three contributing areas were within an <11 km radius of the clinic and accounted for 29.2% of the total patient count, while 96.2% of all admissions arrived from a <50 km range. The selected weather stations are indicated with the icon (
) and Stuttgart. f Geospatial distribution highlighting the density of ischemic strokes per 100,000 population in the catchment area of UMC using the postal code-based distribution of patients’ home locations. The top three contributing areas were within an <11 km radius of the clinic and accounted for 29.2% of the total patient count, while 96.2% of all admissions arrived from a <50 km range. The selected weather stations are indicated with the icon ( ).
).
References
-
- Carlson, C. J. After millions of preventable deaths, climate change must be treated like a health emergency. Nat. Med.30, 622 (2024). - PubMed
LinkOut - more resources
Full Text Sources
