

The dynamic immune behavior of primary and metastatic ovarian carcinoma
- PMID: 40281242
- PMCID: PMC12032089
- DOI: 10.1038/s41698-025-00818-8
The dynamic immune behavior of primary and metastatic ovarian carcinoma
Abstract
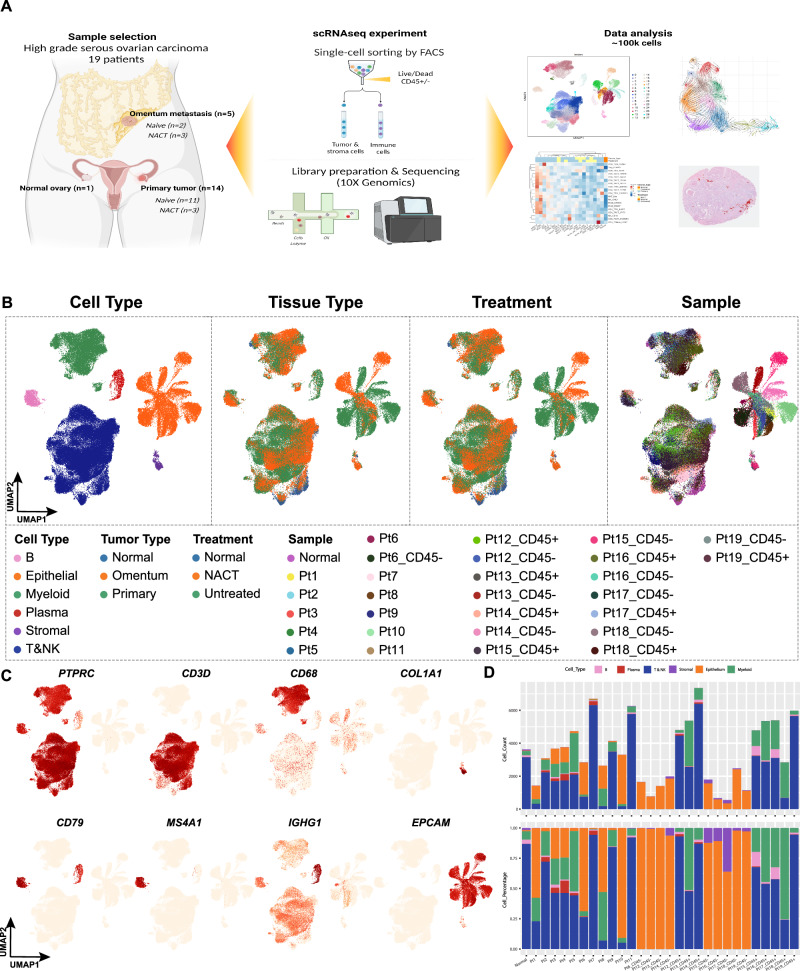
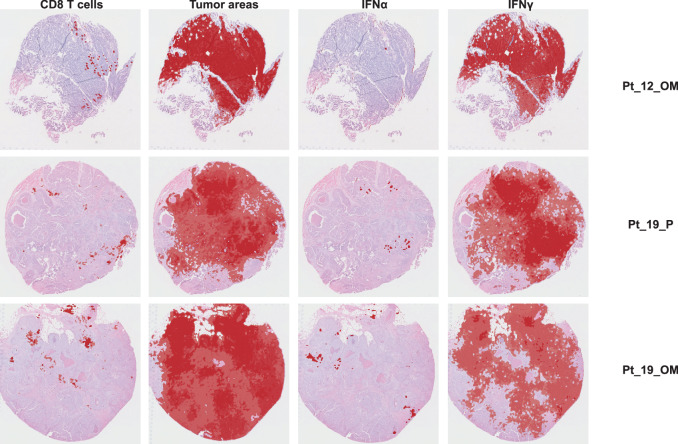
Patients with high-grade serous ovarian carcinoma (HGSC) are usually diagnosed with advanced-stage disease, and the tumors often have immunosuppressive characteristics. Together, these factors are important for disease progression, drug resistance, and mortality. In this study, we used a combination of single-cell sequencing and spatial transcriptomics to identify the molecular mechanisms that lead to immunosuppression in HGSC. Primary tumors consistently showed a more active immune microenvironment than did omental tumors. In addition, we found that untreated primary tumors were mostly populated by dysfunctional CD4 and CD8 T cells in later stages of differentiation; this, in turn, was correlated with expression changes in the interferon α and γ pathways in epithelial cells, showing that cross-communication between the epithelial and immune compartments is important for immune suppression in HGSC. These findings could have implications for the design of clinical trials with immune-modulating drugs.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: A.K.S. is a consultant for Merck, GSK, Astra Zeneca, ImmunoGen, Iylon, Onxeo and DSMB for Advenchen and Mural Oncology. N.D.F. is a consultant for GlaxoSmithKline and Immunogen. S.P.S. reports research funding from AstraZeneca and Bristol Myers Squibb, outside the scope of this work; S.P.S. is a consultant and shareholder of Canexia Health Inc. The other authors declare no competing interests.
Figures



References
-
- Coalition Woc. The World Ovarian Cancer Coalition atlas. The Every Woman Study 2018. https://worldovariancancercoalition.org/wp-content/uploads/2018/10/THE-W...) (2018).
-
- Lheureux, S., Braunstein, M. & Oza, A. M. Epithelial ovarian cancer: Evolution of management in the era of precision medicine. CA Cancer J. Clin.69, 280–304 (2019). - PubMed
-
- Berchuck, A. et al. Patterns of gene expression that characterize long-term survival in advanced stage serous ovarian cancers. Clin. Cancer Res.11, 3686–3696 (2005). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
