

Clinical characteristics and outcomes of acute coronary syndrome patients in a PCI-Limited setting: a prospective study from Bhutan
- PMID: 40281444
- PMCID: PMC12023524
- DOI: 10.1186/s12872-025-04782-w
Clinical characteristics and outcomes of acute coronary syndrome patients in a PCI-Limited setting: a prospective study from Bhutan
Abstract
Introduction: Coronary artery disease is the most prevalent heart condition and a leading cause of mortality worldwide. Acute coronary syndrome (ACS) encompasses ST-elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), and unstable angina (UA). ACS has become an increasingly concerning health issue in Bhutan. Currently, no baseline data exists on ACS in the country. This study aims to assess the burden of ACS by analyzing the clinical characteristics and outcomes of patients diagnosed with ACS who presented to the National Referral Hospital in Bhutan.
Methods: A prospective cohort study was conducted at the Emergency Department of Jigme Dorji Wangchuk (JDW) National Referral Hospital from October 1, 2022, to September 30, 2023. All patients diagnosed with ACS who presented to the Emergency Department were included in the study. Demographic and clinical presentations were recorded. Electrocardiogram (ECG) recordings were performed for all patients with ACS and categorized into STEMI, NSTEMI, and UA. Appropriate treatments were initiated, and patients were closely monitored. Depending on the severity, patients were either admitted to the medical ward or intensive care unit, while some were discharged home. All data were recorded using a standard pro forma developed for the study. Data analysis was performed using SPSS version 23.
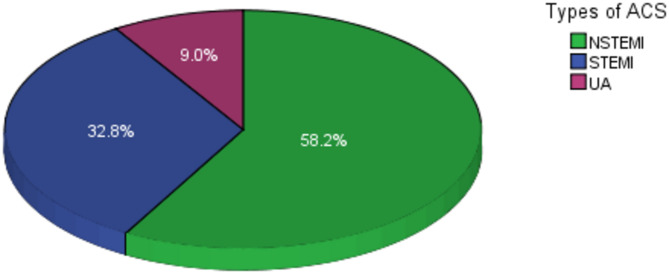
Results: During the study period, 67 patients were diagnosed with ACS. Of these, over 58% (39/67) had NSTEMI, while approximately 33% (22/67) had STEMI. The mean age ± SD of ACS patients was 63.5 ± 16.8 years, with the majority being male (67.2%, 45/67). More than half of the ACS patients presented to the hospital within 24 h of symptom onset, with chest pain (29.7%) and shortness of breath (26.4%) being the most common complaints. Among STEMI patients, over 60% exhibited ST elevation in the anterior and septal leads on ECG, and more than two-thirds required thrombolytic therapy (77.3%, 17/22). Among thrombolytic agents, alteplase was the most commonly used (70%), followed by streptokinase (17.6%). Of the 67 ACS patients, over 46% (31/67) developed complications, with more than one-fourth experiencing heart failure (26.9%). Complications were significantly more common in STEMI patients compared to those with NSTEMI (p < 0.001). The majority (61.2%, 41/67) were discharged home after improvement, while one-third required referral overseas for cardiac interventions. Older age (≥ 60 years) was independently associated with ACS (OR 9.5, 95% CI 1.1-86.9, p = 0.046). Other medical conditions, including hypertension, diabetes, dyslipidemia, and smoking, increased the likelihood of ACS; however, these associations were not statistically significant (p > 0.05).
Conclusion: Among the cases of acute coronary syndrome, 58% were classified as NSTEMI and 33% as STEMI. A majority of patients presented to the hospital within 24 h, expressing complaints of chest pain and shortness of breath, and received essential thrombolytic therapy. Approximately 48% of these patients developed complications, and over one-third were referred overseas for additional treatment. This study indicates that acute coronary syndrome is an emerging public health concern in Bhutan, underscoring the urgent necessity for the establishment of percutaneous coronary intervention (PCI) within the country to mitigate the need for overseas referrals.
Keywords: Acute coronary syndrome; Cardiovascular diseases; Myocardial infarction; ST-elevation myocardial infarction; Thrombolytic therapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Institutional Review Board (IRB) of Khesar Gyalpo University of Medical Sciences of Bhutan (KGUMSB) with Ref No: IRB/Approval/PN/2022-012/946. Written informed consent was obtained from all the study participants. This prospective cohort study was performed in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Clinical trial number: Not applicable.
Figures
References
-
- Task A et al. 2023 ESC Guidelines for the management of acute coronary syndromes Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC) (United Kingdom), (United Kingdom), Takeshi Kimura (Japan), Vi, pp. 3720–3826, 2023, 10.1093/eurheartj/ehad191
-
- NICE. Acute coronary syndromes, NICE guideline. Accessed: Dec. 22, 2024. [Online]. Available: https://www.nice.org.uk/guidance/ng185/resources/acute-coronary-syndrome...
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
