

Impact of physician awareness and microbiological examination on incidence of COVID-19-associated pulmonary aspergillosis: a retrospective study
- PMID: 40281478
- PMCID: PMC12023659
- DOI: 10.1186/s12890-025-03671-4
Impact of physician awareness and microbiological examination on incidence of COVID-19-associated pulmonary aspergillosis: a retrospective study
Abstract
Background: The reported incidence of aspergillosis among COVID-19 patients has varied significantly, which can be partly attributed to differences in diagnostic approaches and levels of physicians' proficiency in diagnosing COVID-19-associated pulmonary aspergillosis (CAPA). Consequently, we conducted a retrospective study to investigate the potential reasons for these discrepancies and analyzed the risk factors for pulmonary aspergillosis in patients with COVID-19.
Method: Data were retrospectively collected from December 1, 2022, to September 30, 2023, from patients who were admitted to the First Affiliated Hospital of Wenzhou Medical University. The research platform was used to screen patients with discharge diagnoses of COVID-19 pneumonia. CAPA was defined according to the 2020 ECMM/ISHAM criteria and the Chinese expert consensus. Clinical data that were collected included data about underlying diseases, laboratory examinations and microbiological detection. Analyses were conducted with R software, with continuous variables analyzed with t-tests, categorical variables analyzed with chi-square tests, and logistic regression and ROC curves used to assess risk factors for CAPA.
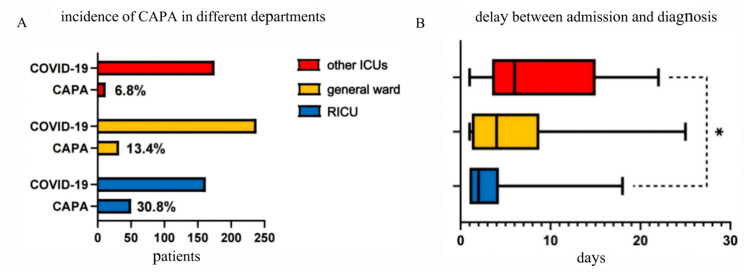
Results: The incidence of CAPA was 13.4% in the general ward, 30.8% in the RICU, and 6.8% in other ICUs. The average time to CAPA diagnosis was 5.6 days in general wards, 3.7 days in the RICU, and 7.4 days in other ICUs. Diagnostic testing revealed the following sensitivities: 78% for BALF galactomannan (GM), 48% for serum GM, 52% for culture tests, and 71% for BALF mNGS. Risk factors for CAPA included chronic respiratory disease, chronic renal insufficiency, and diabetes. The primary Aspergillus species identified was A. fumigatus, followed by A. flavus.
Conclusion: Differences in incidence may arise from varying levels of physician awareness, which can influence the rate at which BALF and serum GM samples are submitted for testing. The sensitivity of BALF GM is higher than that of serum GM. Furthermore, BALF mNGS has the potential to enhance the clinical detection sensitivity of CAPA. Risk factors for CAPA include chronic respiratory disease, chronic renal insufficiency, and diabetes, which may aid in identifying at-risk patients. The primary Aspergillus species identified was A. fumigatus, followed by A. flavus, providing a reference for clinical empirical treatment.
Clinical trial number: Not applicable.
Keywords: A. fumigatus; BALF GM; BALF mNGS; CAPA; General wards; Incidence; Other ICUs; RICU; Serum GM.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was conducted in accordance with the Declaration of Helsinki (revised in 2013), approved by the Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (KY2024-R216) and the informed consent was waived. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
