

Combined Risk Stratification With Patient Characteristics and Biomarkers in Patients Treated With the Impella for Cardiogenic Shock
- PMID: 40281652
- PMCID: PMC12184222
- DOI: 10.1161/JAHA.124.040487
Combined Risk Stratification With Patient Characteristics and Biomarkers in Patients Treated With the Impella for Cardiogenic Shock
Abstract
Background: In patients with cardiogenic shock (CS), a percutaneous microaxial ventricular assist device (Impella, Abiomed, Danvers, MA) is a choice for temporary mechanical circulatory support. Given the high morbidity and mortality in this patient population, early risk stratification is relevant when making treatment decisions.
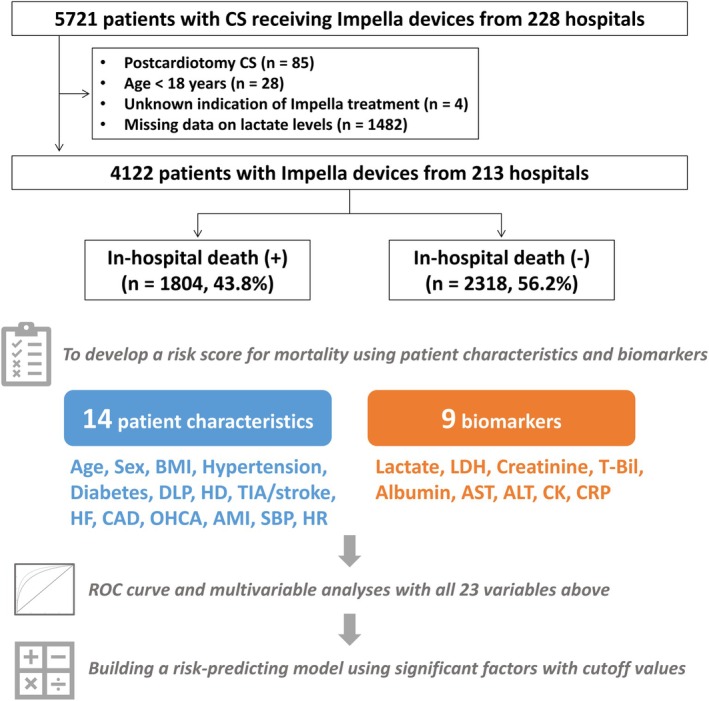
Methods: Using nationwide registry data between February 2020 and December 2022 in Japan, we included a total of 4122 patients with cardiogenic shock treated with the Impella devices. Using logistic regression analysis, we incorporated patient characteristics and biomarkers to develop a risk-stratifying model for in-hospital mortality. The model was also tested if applicable to composite outcomes of in-hospital death and major complications.
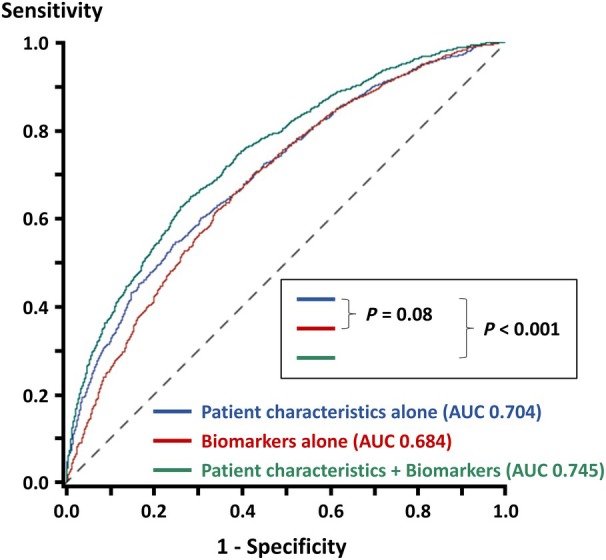
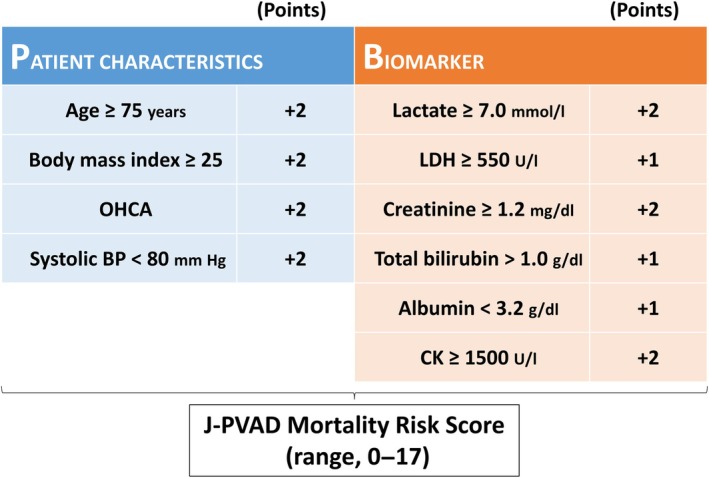
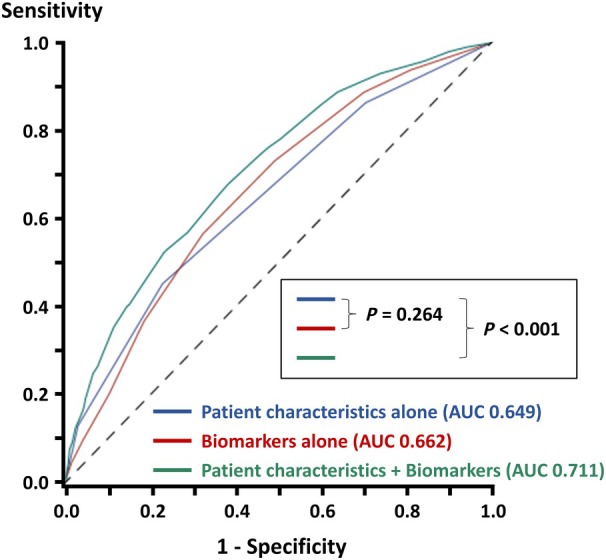
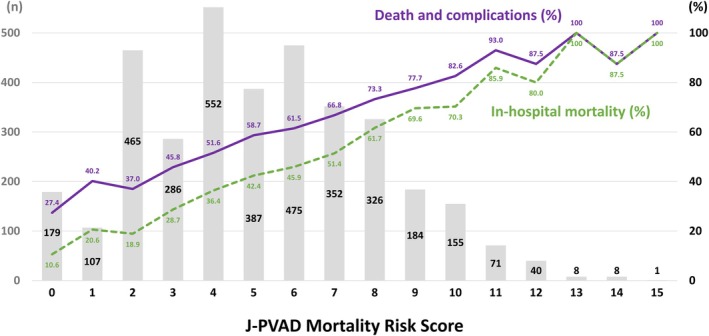
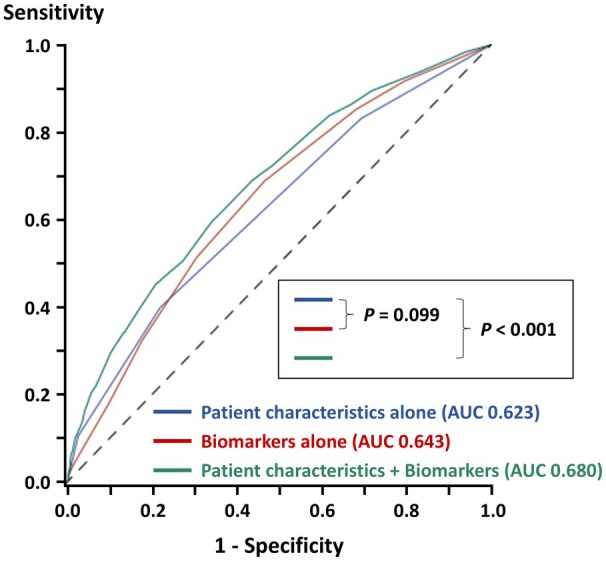
Results: Of the 4122 patients with cardiogenic shock, the Impella was indicated for acute myocardial infarction in 2575 (62.5%). Multivariable analysis identified 4 patient characteristics (age, body mass index, out-of-hospital cardiac arrest, and blood pressure) and 6 biomarkers (lactate, lactate dehydrogenase, creatinine, total bilirubin, albumin, and creatinine kinase) with cutoff values as factors significantly associated with in-hospital mortality. We developed a risk-stratifying model using the 10 variables, which was predictive of in-hospital death (area under the curve, 0.711; P<0.001). Adding biomarkers to patient characteristics significantly improved the diagnostic accuracy (area under the curve, from 0.649 to 0.711; P<0.001). This risk score was also predictive of death and major complications (area under the curve, 0.680; P<0.001).
Conclusions: In patients with cardiogenic shock treated with the Impella devices, our risk-stratifying system, consisting of 4 patient characteristics and 6 biomarkers, strongly correlated with in-hospital mortality, potentially facilitating clinical decision-making.
Keywords: Impella; cardiogenic shock; mechanical circulatory support; risk stratification.
Conflict of interest statement
Dr Koichi Toda reports speaker fees from Abiomed Japan. Dr Yoshio Kobayashi reports honoraria from Abiomed Japan. The remaining authors have no disclosures to report.
Figures
References
-
- Naidu SS, Baran DA, Jentzer JC, Hollenberg SM, van Diepen S, Basir MB, Grines CL, Diercks DB, Hall S, Kapur NK, et al. SCAI SHOCK Stage Classification Expert Consensus Update: a review and incorporation of validation studies: this statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J Am Coll Cardiol. 2022;79:933–946. doi: 10.1016/j.jacc.2022.01.018 - DOI - PubMed
-
- Geller BJ, Sinha SS, Kapur NK, Bakitas M, Balsam LB, Chikwe J, Klein DG, Kochar A, Masri SC, Sims DB, et al. Escalating and de‐escalating temporary mechanical circulatory support in cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2022;146:e50–e68. doi: 10.1161/CIR.0000000000001076 - DOI - PubMed
-
- Balthazar T, Vandenbriele C, Verbrugge FH, Den Uil C, Engström A, Janssens S, Rex S, Meyns B, Van Mieghem N, Price S, et al. Managing patients with short‐term mechanical circulatory support: JACC review topic of the week. J Am Coll Cardiol. 2021;77:1243–1256. doi: 10.1016/j.jacc.2020.12.054 - DOI - PubMed
-
- Saito S, Okubo S, Matsuoka T, Hirota S, Yokoyama S, Kanazawa Y, Takei Y, Tezuka M, Tsuchiya G, Konishi T, et al. Impella—current issues and future expectations for the percutaneous, microaxial flow left ventricular assist device. J Cardiol. 2024;83:228–235. doi: 10.1016/j.jjcc.2023.10.008 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
