

Comparing the Prognostic Value of Quantitative Response Assessment Tools and LIRADS Treatment Response Algorithm in Patients with Hepatocellular Carcinoma Following Interstitial High-Dose-Rate Brachytherapy and Conventional Transarterial Chemoembolization
- PMID: 40282451
- PMCID: PMC12025668
- DOI: 10.3390/cancers17081275
Comparing the Prognostic Value of Quantitative Response Assessment Tools and LIRADS Treatment Response Algorithm in Patients with Hepatocellular Carcinoma Following Interstitial High-Dose-Rate Brachytherapy and Conventional Transarterial Chemoembolization
Abstract
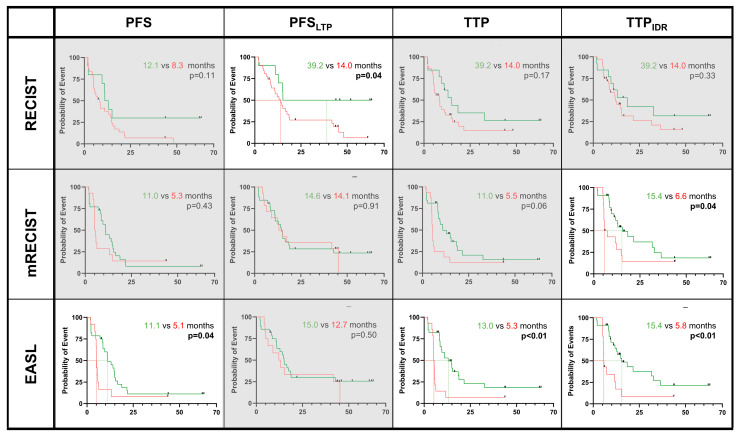
Background/Objectives: The aim of this study was to investigate the prognostic value of established response assessment tools for hepatocellular carcinoma (HCC) treated with high-dose-rate interstitial brachytherapy (iBT) alone or with transarterial chemoembolization (cTACE). Methods: (Non-)responders were categorized using size-based RECIST 1.1 and WHO criteria, enhancement-based mRECIST and EASL criteria, and the LI-RADS Treatment Response Algorithm (LR-TRA). The outcomes were the overall survival (OS), progression-free survival (PFS), and time to progression (TTP). The statistics used included Fisher's exact test, a t-test, the Mann-Whitney-U test, and a Kaplan-Meier analysis. The median OS, PFS, and TTP were higher in patients following iBT (26.3, 9.1, and 13.0 months) than following cTACE/iBT (23.3, 7.6, and 9.2 months). Results: The enhancement-based criteria identified more responders and predicted PFS and TTP better compared to the size-based criteria. At two months, the cTACE/iBT responders showed improved PFS (mRECIST and EASL: 11.3 vs. 2.3 and 11.0 vs. 2.3, p < 0.01) and TTP (mRECIST and EASL: 11.9 vs. 2.4 months, p < 0.01) by the enhancement-based criteria. An EASL assessment at five months predicted improved survival following both cTACE/iBT (PFS: 11.9 vs. 5.1 months, p = 0.03; TTP: 12.4 vs. 5.0, p < 0.01) and iBT (11.1 vs. 5.1 months, p = 0.04; 13.0 vs. 5.3, p < 0.01). The LR-TRA showed OS benefits at five months for cTACE/iBT responders. Size-based criteria were not prognostic. Conclusions: Extending follow-up post-iBT or post-iBT/cTACE may improve responder stratification and prognostication.
Keywords: LIRADS Treatment Response Algorithm; hepatocellular carcinoma; interstitial brachytherapy; locoregional therapies; response assessment; transarterial chemoembolization.
Conflict of interest statement
The authors do not declare any conflicts of interest. Outside the submitted work, L.J.S. received funding from the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG): CRC 1340 “Matrix in vision”—Project-ID 372486779; research unit FOR5628 “Onco-MRE”. L.J.S. received research grants from the Berliner Krebsgesellschaft e.V., Charité 3R, and research grants and honoraria from Guerbet. F.H., C.A.H. and L.J.S. are fellows of the BIH (Junior Digital) Clinician Scientist Program funded by the Charité–Universitätsmedizin Berlin and the Berlin Institute of Health. Y.H. received stipends from the Chinese Scholar Council. E.Y.Y. received a stipend from the Fuldt Stiftung. T.P. receives funding from Berlin Institute of Health (Advanced Clinician Scientist Grant, Platform Grant), Ministry of Education and Research (BMBF, 01KX2021 (RACOON), 01KX2121 (XNUM 2.0′, RACOON), 68GX21001A, 01ZZ2315D), German Research Foundation (DFG, SFB 1340/2), European Union (H2020, CHAIMELEON: 952172, DIGITAL, EUCAIM: 101100633) and reports research agreements (no personal payments, outside of submitted work) with AGO, Aprea AB, ARCAGY-GINECO, Astellas Pharma Global Inc. (APGD), Astra Zeneca, Clovis Oncology, Inc., Holaira, Incyte Corporation, Karyopharm, Lion Biotechnologies, Inc., MedImmune, Merck Sharp & Dohme Corp, Millennium Pharmaceuticals, Inc., Morphotec Inc., NovoCure Ltd., PharmaMar S.A. and PharmaMar USA, Inc., Roche, Siemens Healthineers, and TESARO Inc., and fees for a book translation (Elsevier B.V.). B.G. receives payment for lectures from Parexel/Calyx, C. R. Bard/BD, Sirtex Medical, St. Jude Medical, Cook, AngioDynamics, Pharmcept, Guerbet, Ewimed, Boston Scientific, Terumo, Roche,Merck, 3M, Beacon Bioscience/ICON, Ipsen, Bayer, Pfizer, Eisai, MSD, Inari, and Siemens/Varian.
Figures



Similar articles
-
Decision-Tree Models Indicative of Microvascular Invasion on MRI Predict Survival in Patients with Hepatocellular Carcinoma Following Tumor Ablation.J Hepatocell Carcinoma. 2024 Jul 3;11:1279-1293. doi: 10.2147/JHC.S454487. eCollection 2024. J Hepatocell Carcinoma. 2024. PMID: 38974016 Free PMC article.
-
Which Criteria Applied in Multi-Phasic CT Can Predict Early Tumor Response in Patients with Hepatocellular Carcinoma Treated Using Conventional TACE: RECIST, mRECIST, EASL or qEASL?Cardiovasc Intervent Radiol. 2018 Mar;41(3):433-442. doi: 10.1007/s00270-017-1829-4. Epub 2017 Oct 30. Cardiovasc Intervent Radiol. 2018. PMID: 29086058 Free PMC article.
-
Combination Therapy of Chemoembolization and Hepatic Arterial Infusion Chemotherapy in Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis Compared with Chemoembolization Alone: A Propensity Score-Matched Analysis.Biomed Res Int. 2021 Jul 14;2021:6670367. doi: 10.1155/2021/6670367. eCollection 2021. Biomed Res Int. 2021. PMID: 34337041 Free PMC article.
-
Single medium-sized hepatocellular carcinoma treated with sequential conventional transarterial chemoembolization (cTACE) and microwave ablation at 4 weeks versus cTACE alone: a propensity score.World J Surg Oncol. 2022 Jun 10;20(1):192. doi: 10.1186/s12957-022-02643-w. World J Surg Oncol. 2022. PMID: 35689233 Free PMC article.
-
Prognostic Relevance of Objective Response According to EASL Criteria and mRECIST Criteria in Hepatocellular Carcinoma Patients Treated with Loco-Regional Therapies: A Literature-Based Meta-Analysis.PLoS One. 2015 Jul 31;10(7):e0133488. doi: 10.1371/journal.pone.0133488. eCollection 2015. PLoS One. 2015. PMID: 26230853 Free PMC article.
Cited by
-
LINC01559: roles, mechanisms, and clinical implications in human cancers.Hum Cell. 2025 Apr 9;38(3):83. doi: 10.1007/s13577-025-01218-7. Hum Cell. 2025. PMID: 40205068 Review.
References
-
- Reig M., Forner A., Rimola J., Ferrer-Fàbrega J., Burrel M., Garcia-Criado Á., Kelley R.K., Galle P.R., Mazzaferro V., Salem R., et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022;76:681–693. doi: 10.1016/j.jhep.2021.11.018. - DOI - PMC - PubMed
-
- Vogel A., Cervantes A., Chau I., Daniele B., Llovet J.M., Meyer T., Nault J.-C., Neumann U., Ricke J., Sangro B., et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018;29((Suppl. S4)):iv238–iv255. doi: 10.1093/annonc/mdy308. - DOI - PubMed
LinkOut - more resources
Full Text Sources
