

Breaking Myths: Comparable Outcomes in Lymph Node Analysis Across Surgical Methods
- PMID: 40282488
- PMCID: PMC12025904
- DOI: 10.3390/cancers17081312
Breaking Myths: Comparable Outcomes in Lymph Node Analysis Across Surgical Methods
Abstract
Background/objectives: Colorectal cancer is the third most common cancer worldwide, making lymph node recovery critical for treatment decisions and prognosis. The relationship between body mass index (BMI) and the number of lymph nodes retrieved during laparoscopic and open surgeries remains controversial. This study aimed to evaluate whether surgical approach and BMI influence lymph node retrieval in colon cancer surgeries.
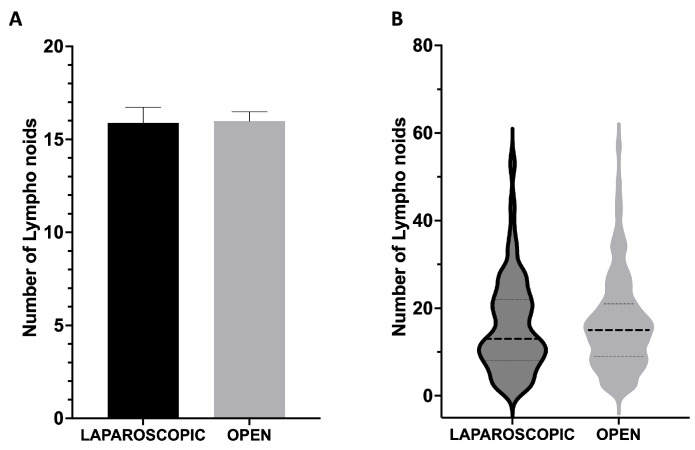
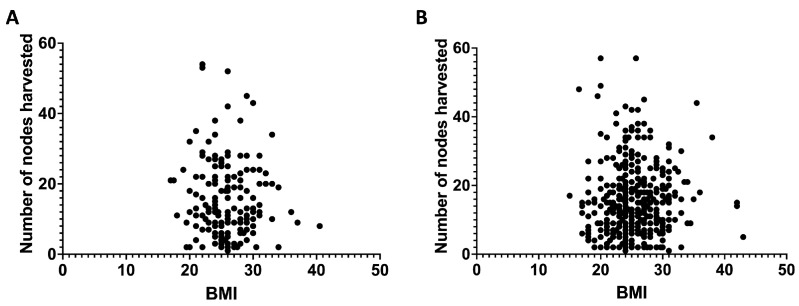
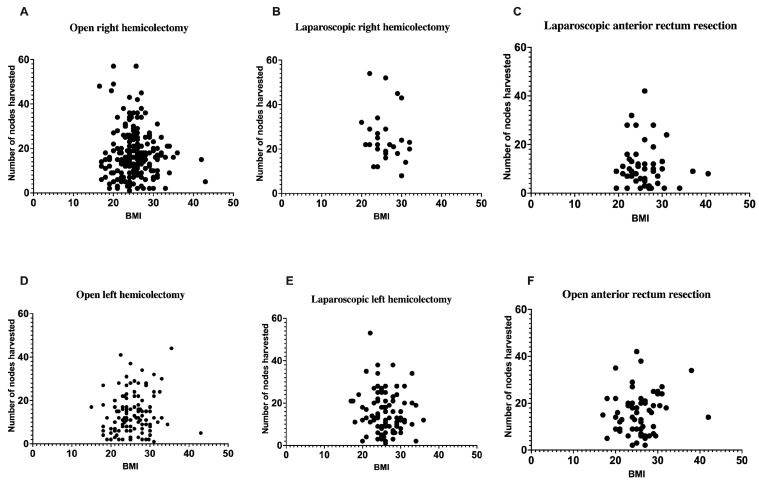
Methods: A retrospective analysis was conducted on 560 patients who underwent colon cancer surgery at a single institution between 2018 and 2023. The average number of lymph nodes retrieved during laparoscopic and open procedures was compared. Distribution analysis using violin plots was performed to assess the pattern of lymph node yield between surgical approaches. Additionally, the impact of BMI on lymph node recovery was assessed. All surgeries were performed by a standardized surgical team using consistent fat clearance techniques.
Results: The mean number of lymph nodes retrieved was 15.89 ± 0.84 for laparoscopic surgeries and 15.98 ± 0.50 for open surgeries, with no statistically significant difference (p = 0.9166). The violin plot analysis confirmed overlapping distributions between the two surgical approaches, with no significant difference (p = 0.6270). BMI also showed no significant effect on the number of lymph nodes removed during surgery. The consistency in outcomes was attributed to standardized surgical practices across all cases.
Conclusions: Laparoscopic and open surgical approaches yield comparable lymph node recovery in colon cancer surgeries, both in terms of mean values and overall distribution patterns, regardless of patient BMI. These findings emphasize the importance of standardized surgical techniques in ensuring reliable outcomes and suggest that both approaches are equally effective in meeting oncological standards for lymph node retrieval.
Keywords: body mass index; colorectal cancer; fat clearance techniques; laparoscopic surgery; lymph nodes.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Factors that influence lymph node retrieval in the surgical treatment of colorectal cancer: a comparison of the laparoscopic versus open approach.Am J Surg. 2013 Mar;205(3):339-42; discussion 342. doi: 10.1016/j.amjsurg.2012.11.003. Am J Surg. 2013. PMID: 23414957
-
Does a laparoscopic approach affect the number of lymph nodes harvested during curative surgery for colorectal cancer?Surg Endosc. 2010 Jan;24(1):113-8. doi: 10.1007/s00464-009-0534-z. Epub 2009 Jun 11. Surg Endosc. 2010. PMID: 19517186
-
Laparoscopic colectomies associated with decreased retrieval of 12 or more lymph nodes compared to open in elective colon cancer surgery.Ecancermedicalscience. 2019 Oct 14;13:968. doi: 10.3332/ecancer.2019.968. eCollection 2019. Ecancermedicalscience. 2019. PMID: 31921339 Free PMC article.
-
Increased fat content and body shape have little effect on the accuracy of lymph node retrieval and blood loss in laparoscopic distal gastrectomy for gastric cancer.J Gastrointest Surg. 2009 Apr;13(4):626-33. doi: 10.1007/s11605-008-0768-4. Epub 2008 Dec 17. J Gastrointest Surg. 2009. PMID: 19089516
-
Are we achieving the benchmark of retrieving 12 lymph nodes in colorectal carcinoma specimens? Experience from a tertiary referral center in India and review of literature.Indian J Pathol Microbiol. 2012 Jan-Mar;55(1):38-42. doi: 10.4103/0377-4929.94853. Indian J Pathol Microbiol. 2012. PMID: 22499298 Review.
References
-
- Carr P.R., Weigl K., Edelmann D., Jansen L., Chang-Claude J., Brenner H., Hoffmeister M. Estimation of Absolute Risk of Colorectal Cancer Based on Healthy Lifestyle, Genetic Risk, and Colonoscopy Status in a Population-Based Study. Gastroenterology. 2020;159:129–138.e9. doi: 10.1053/j.gastro.2020.03.016. - DOI - PMC - PubMed
-
- Richardson A., Hayes J., Frampton C., Potter J. Modifiable Lifestyle Factors That Could Reduce the Incidence of Colorectal Cancer in New Zealand. NZ Med. J. 2016;129:13–20. - PubMed
LinkOut - more resources
Full Text Sources
