

Adjuvant Therapy in "Intermediate-Risk" Early-Stage Cervical Cancer: To Treat or Not to Treat? Systematic Review and Meta-Analysis
- PMID: 40282496
- PMCID: PMC12026193
- DOI: 10.3390/cancers17081320
Adjuvant Therapy in "Intermediate-Risk" Early-Stage Cervical Cancer: To Treat or Not to Treat? Systematic Review and Meta-Analysis
Abstract
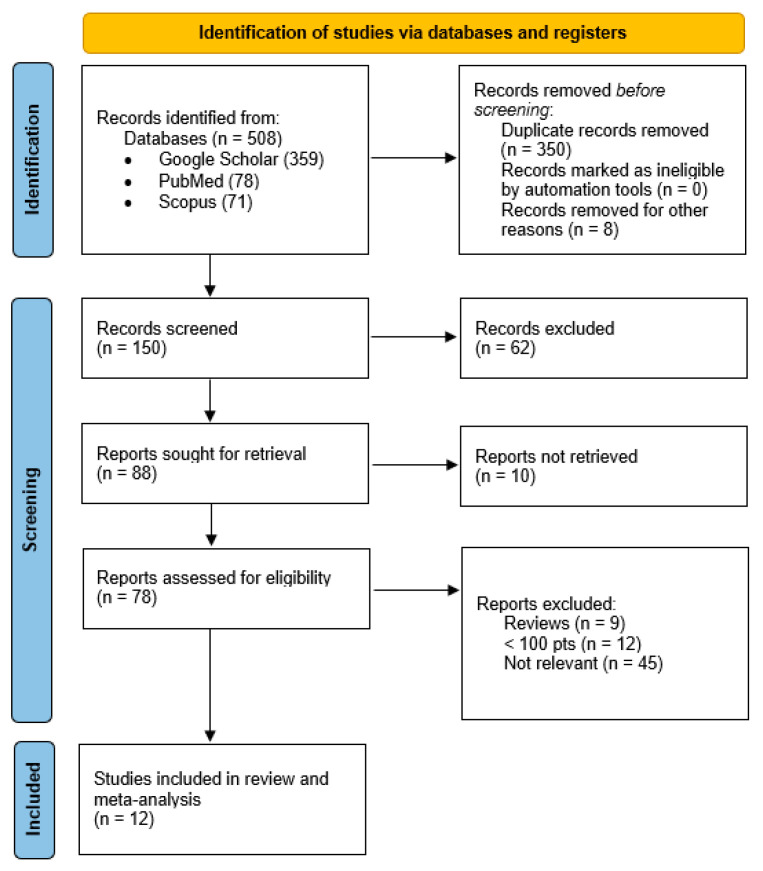
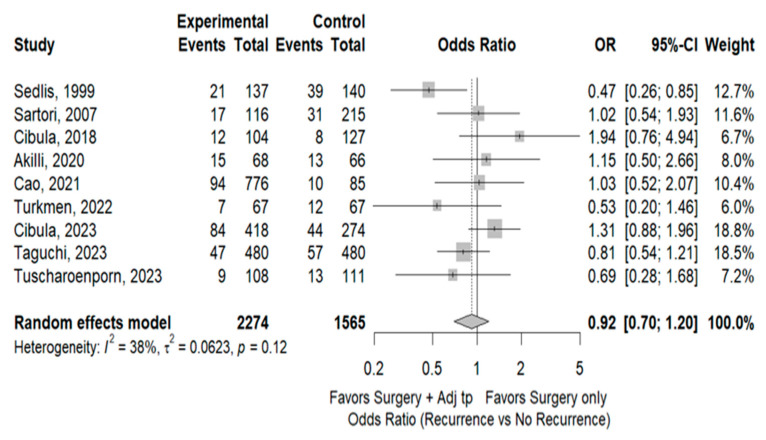
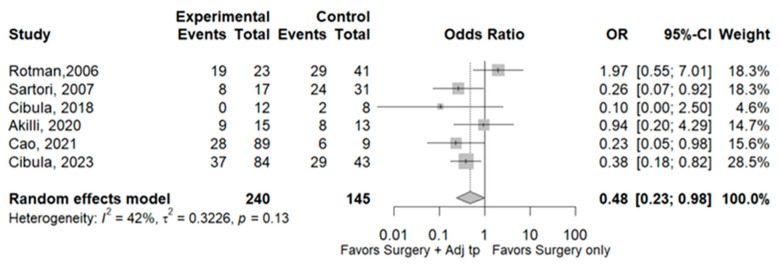
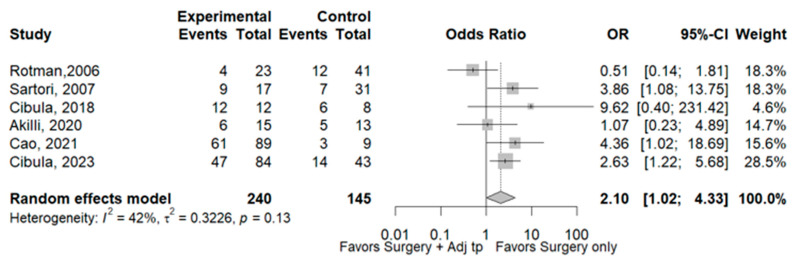
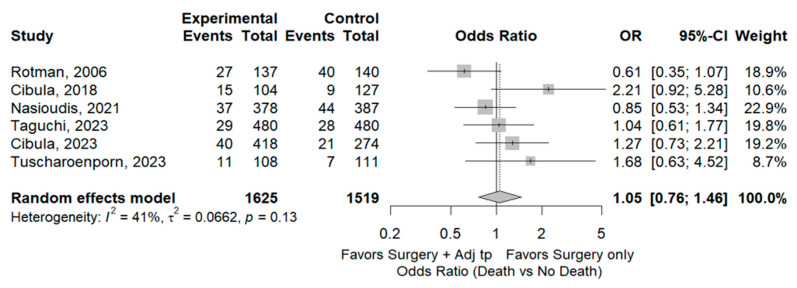
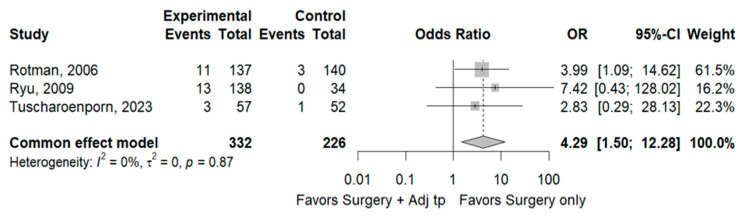
International guidelines do not take a clear position regarding the management of patients with "intermediate-risk" cervical cancer, and they remain noncommittal on the necessity of adjuvant therapy following radical hysterectomy. To determine if adjuvant therapy after surgery adds benefit in "intermediate-risk" cervical cancer patients in terms of recurrence rate and mortality rate, we performed a systematic review with meta-analysis on Google Scholar, PubMed, and Scopus. The inclusion criteria were studies with >100 patients with intermediate-risk cervical cancer according to the Sedlis criteria, RCTs, or propensity score-matched cohort studies reporting oncological outcomes and treatment-related toxicity, comparing a surgery-only cohort with an adjuvant therapy cohort. We found 11 studies that met our inclusion criteria, comprising a total of 4011 patients. The mean follow-up was 80.7 months. No statistically significant differences were found for both outcomes, respectively, recurrence rate OR 0.92 (95% CI 0.70-1.20, I2 38%) and mortality rate OR 1.05 (95% CI 0.77-1.46, I2 41%). However, a statistically significant difference was found in the site of recurrence-pelvic OR 0.48 (95% CI 0.23-0.98, p < 0.001, I2 42%) or distant OR 2.10 (95% CI 1.02-4.33, p < 0.001 I2 42%). Treatment-related risk of Grade 3 or 4 toxicity was statistically significant. Our meta-analysis shows that oncological outcomes in this class of patients are similar between the two groups. However, while awaiting the results of new RCTs, it is crucial to define a personalized diagnostic and therapeutic strategy for each patient.
Keywords: ajuvant therapy; ater surgery treatment; intermediate-risk early-stage cervical cancer; radiotherapy; surgery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
The effect of adjuvant radiotherapy on oncological outcomes in patients with early-stage cervical carcinoma with only intermediate-risk factors: a propensity score matching analysis.J Obstet Gynaecol. 2022 Oct;42(7):3204-3211. doi: 10.1080/01443615.2022.2109406. Epub 2022 Aug 12. J Obstet Gynaecol. 2022. PMID: 35959796
-
Adjuvant Radiotherapy for Intermediate-Risk Early-Stage Cervical Cancer Post Radical Hysterectomy: A Systematic Review and Meta-Analysis.J Clin Med. 2025 Jun 5;14(11):4002. doi: 10.3390/jcm14114002. J Clin Med. 2025. PMID: 40507766 Free PMC article. Review.
-
Adjuvant therapy in early-stage cervical cancer after radical hysterectomy: are we overtreating our patients? A meta-analysis.Clin Transl Oncol. 2022 Aug;24(8):1605-1614. doi: 10.1007/s12094-022-02808-9. Epub 2022 Apr 19. Clin Transl Oncol. 2022. PMID: 35441353 Review.
-
Efficacy and safety analysis of non-radical surgery for early-stage cervical cancer (IA2 ~ IB1): a systematic review and meta-analysis.Front Med (Lausanne). 2024 Apr 30;11:1337752. doi: 10.3389/fmed.2024.1337752. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38745744 Free PMC article.
-
Post-operative small pelvic field radiation therapy in patients with intermediate risk early stage cervix cancer: a safe and efficient treatment modality.Rep Pract Oncol Radiother. 2021 Jun 9;26(3):360-366. doi: 10.5603/RPOR.a2021.0043. eCollection 2021. Rep Pract Oncol Radiother. 2021. PMID: 34277089 Free PMC article.
References
-
- Cibula D., Raspollini M.R., Planchamp F., Centeno C., Chargari C., Felix A., Fischerová D., Jahnn-Kuch D., Joly F., Kohler C., et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer—Update 2023*. Int. J. Gynecol. Cancer. 2023;33:649–666. doi: 10.1136/ijgc-2023-004429. - DOI - PMC - PubMed
-
- Cibula D., Akilli H., Jarkovsky J., van Lonkhuijzen L., Scambia G., Meydanli M.M., Ortiz D.I., Falconer H., Abu-Rustum N.R., Odetto D., et al. Role of adjuvant therapy in intermediate-risk cervical cancer patients—Subanalyses of the SCCAN study. Gynecol. Oncol. 2023;170:195–202. doi: 10.1016/j.ygyno.2023.01.014. - DOI - PMC - PubMed
-
- Sedlis A., Bundy B.N., Rotman M.Z., Lentz S.S., Muderspach L.I., Zaino R.J. A Randomized Trial of Pelvic Radiation Therapy versus No Further Therapy in Selected Patients with Stage IB Carcinoma of the Cervix after Radical Hysterectomy and Pelvic Lymphadenectomy: A Gynecologic Oncology Group Study. Gynecol. Oncol. 1999;73:177–183. doi: 10.1006/gyno.1999.5387. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
