

A Single Port (SP) Approach Reduces the Risk of Postoperative Complications in Elderly Patients Undergoing Robotic-Assisted Partial Nephrectomy (RAPN)
- PMID: 40282500
- PMCID: PMC12026311
- DOI: 10.3390/cancers17081324
A Single Port (SP) Approach Reduces the Risk of Postoperative Complications in Elderly Patients Undergoing Robotic-Assisted Partial Nephrectomy (RAPN)
Abstract
Introduction: In recent years, due to the increasing life expectancy and the growing popularity of nephron sparing strategies (NSS), more elderly and frail patients are undergoing Robotic-Assisted Partial Nephrectomy (RAPN) for the treatment of localized Renal Cell Carcinoma (RCC). A Single Port Approach has demonstrated itself to reduce estimated blood loss (EBL), complication rates, and length of stay (LOS). In the present study, we aim to compare perioperative and postoperative outcomes of SP RAPN and Multi Port (MP) RAPN, with a focus on elderly patients.
Materials and methods: In the study, 293 cN0M0 RCC patients who underwent MP and SP RAPN performed at our institution from 2018 to 2024 were retrospectively reviewed. Clinical, demographic, patient, and tumor characteristics and perioperative variables were assessed across group A (<65 years old) and group B (≥65 years old) patients, as well as MP and SP cohorts. Subsequently, univariate and multivariate regression analyses were carried out, particularly for elderly patients, to evaluate the impact of selected preoperative and perioperative variables on the risk of 30-day postoperative complications.
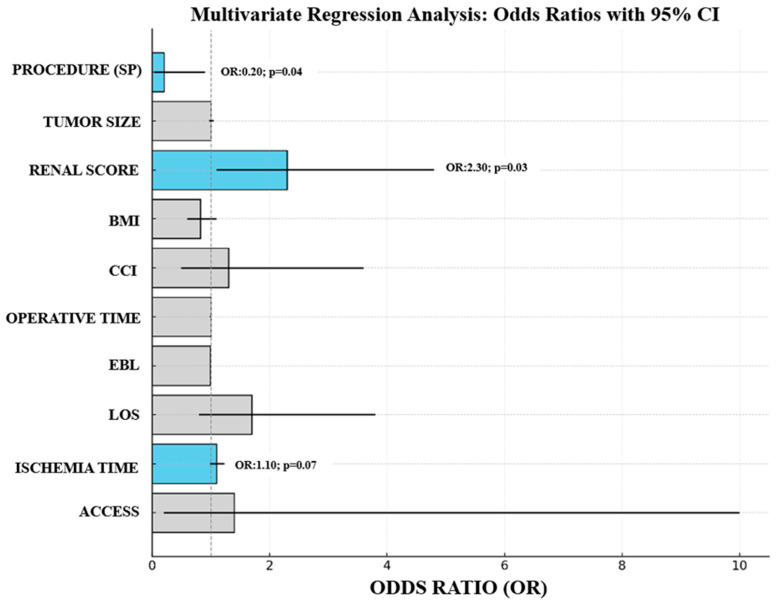
Results: Clinical and demographic characteristics were similar across the MP and SP cohorts of group A and group B. The SP cohort of both group A and group B demonstrated significantly higher rates of extraperitoneal access (75.9% vs. 26.6% for group A, p < 0.001 and 81.8% vs. 26.2% for group B, p < 0.001), shorter median operative times (186 [142.8-222] min vs. 190 [153-238] min for group A, p < 0.001 and 173.5 [143-228] min vs. 206 [178-237] min for group B, p < 0.001), and shorter median LOS (0 [0-1] days vs. 2 [1-3] days for group A, p < 0.001 and 0 [0,1] days vs. 2 [2-4] days for group B, p < 0.001). Moreover, for both groups, an SP approach required significantly longer median ischemia times (21 min [18-31] vs. 20 min [16-24] for group A, p = 0.02 and 24.5 min [20-28] vs. 19.5 min [16-26] for group B, p = 0.03). However, the SP cohort of group B, despite the lower rate of on-clamp procedures (63.4% vs. 90.5%, p = 0.03), demonstrated significantly lower median EBL (50 mL [31-142] vs. 100 mL [50-200], p = 0.03). At multivariate analysis, the SP approach was an independent predictor of lower 30-day postoperative complications (OR: 0.2, 95%CI 0.04-0.9, p = 0.04).
Conclusions: In the present study, elderly patients undergoing SP RAPN did not demonstrate higher complication rates, EBL or hospitalization days compared to their younger counterparts. Moreover, an SP approach was found protective for 30-day postoperative complications. Our results suggest that SP RAPN is feasible and safe in older and frailer patients.
Keywords: Robotic-Assisted Partial Nephrectomy (RAPN); Single Port (SP); ccomplications; elderly.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Comparative outcomes of multi-port versus single-port robotic-assisted partial nephrectomy with same-day discharge: impact of surgical approach.J Robot Surg. 2025 Jul 11;19(1):374. doi: 10.1007/s11701-025-02522-y. J Robot Surg. 2025. PMID: 40643740
-
Single-port vs multi-port robot-assisted partial nephrectomy: A single center propensity score-matched analysis.Eur J Surg Oncol. 2024 Mar;50(3):108011. doi: 10.1016/j.ejso.2024.108011. Epub 2024 Feb 8. Eur J Surg Oncol. 2024. PMID: 38359726
-
Single-Port vs Multiport Robot-Assisted Partial Nephrectomy: A Meta-Analysis.J Endourol. 2024 Mar;38(3):253-261. doi: 10.1089/end.2023.0505. Epub 2024 Feb 13. J Endourol. 2024. PMID: 38185840
-
Perioperative and oncologic outcomes of single-port versus conventional robotic-assisted partial nephrectomy: an evidence-based analysis of comparative outcomes.J Robot Surg. 2023 Jun;17(3):765-777. doi: 10.1007/s11701-022-01491-w. Epub 2022 Dec 5. J Robot Surg. 2023. PMID: 36469187 Review.
-
Single-Port robot assisted partial nephrectomy: initial experience and technique with the da Vinci Single-Port platform (IDEAL Phase 1).Minerva Urol Nephrol. 2022 Apr;74(2):216-224. doi: 10.23736/S2724-6051.21.03919-9. Epub 2021 Mar 26. Minerva Urol Nephrol. 2022. PMID: 33769009 Review.
References
-
- Gray R.E., Harris G.T. Renal Cell Carcinoma: Diagnosis and Management. Am. Fam. Physician. 2019;99:179–184. - PubMed
-
- Vasudev N.S., Wilson M., Stewart G.D., Adeyoju A., Cartledge J., Kimuli M., Datta S., Hanbury D., Hrouda D., Oades G., et al. Challenges of early renal cancer detection: Symptom patterns and incidental diagnosis rate in a multicentre prospective UK cohort of patients presenting with suspected renal cancer. BMJ Open. 2020;10:e035938. doi: 10.1136/bmjopen-2019-035938. - DOI - PMC - PubMed
-
- Roos F.C., Steffens S., Junker K., Janssen M., Becker F., Wegener G., Brenner W., Steinestel J., Schnoeller T.J., Schrader M., et al. Survival advantage of partial over radical nephrectomy in patients presenting with localized renal cell carcinoma. BMC Cancer. 2014;14:372. doi: 10.1186/1471-2407-14-372. - DOI - PMC - PubMed
-
- Ljungberg B., Albiges L., Abu-Ghanem Y., Bedke J., Capitanio U., Dabestani S., Fernández-Pello S., Giles R.H., Hofmann F., Hora M., et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022;82:399–410. doi: 10.1016/j.eururo.2022.03.006. - DOI - PubMed
LinkOut - more resources
Full Text Sources
