

Aggressive Squamoid Eccrine Ductal Carcinoma of the Face: A Rare and Challenging Diagnosis-Case Report and Literature Review
- PMID: 40282903
- PMCID: PMC12028541
- DOI: 10.3390/medicina61040612
Aggressive Squamoid Eccrine Ductal Carcinoma of the Face: A Rare and Challenging Diagnosis-Case Report and Literature Review
Abstract
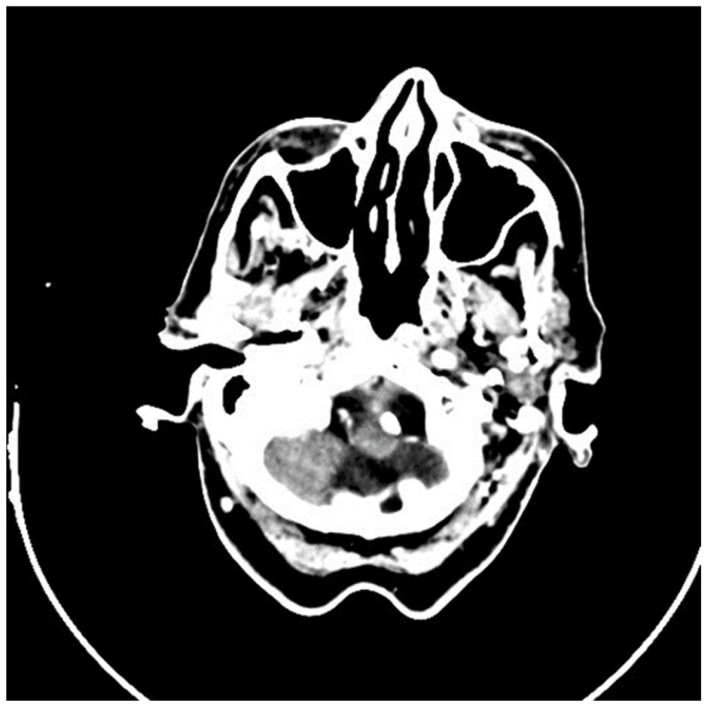
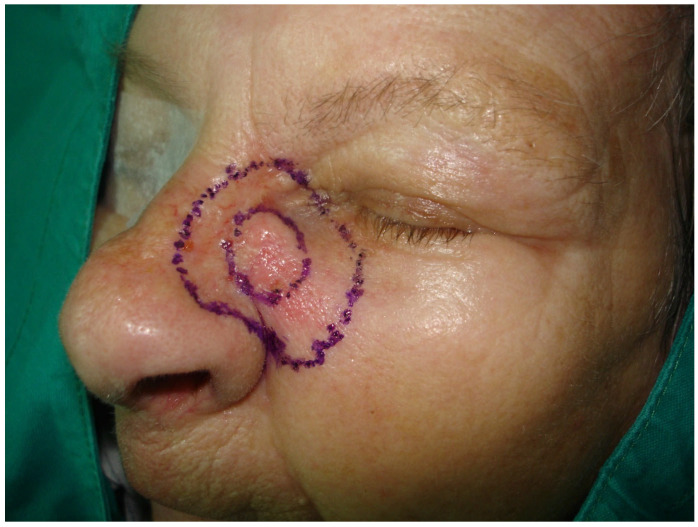
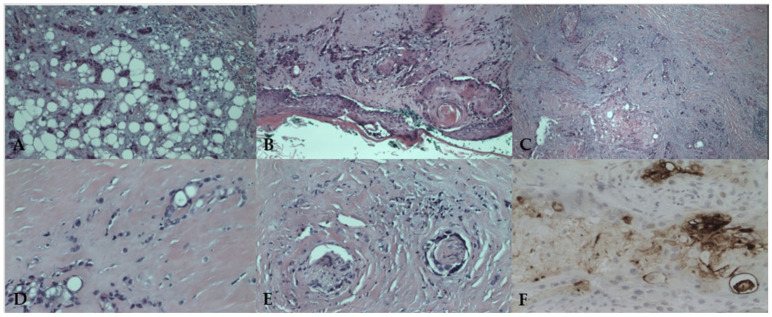
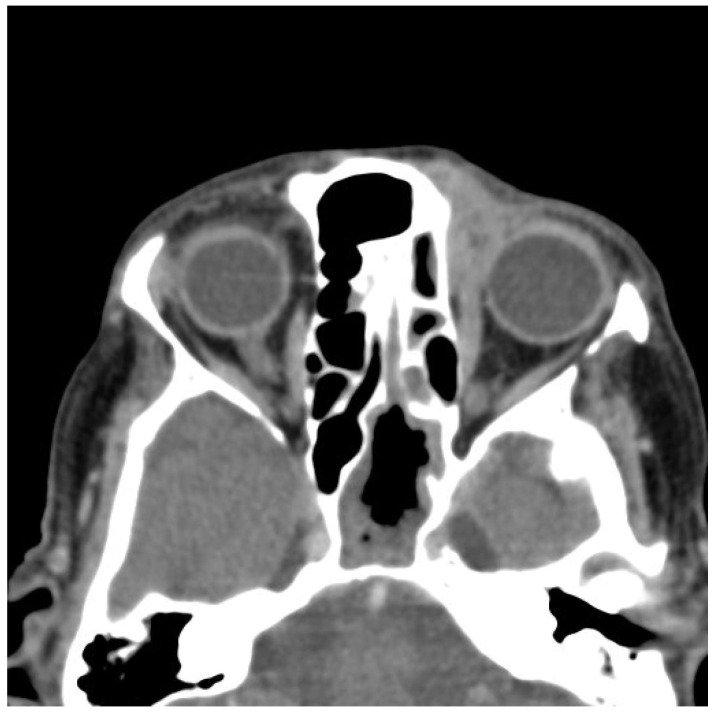
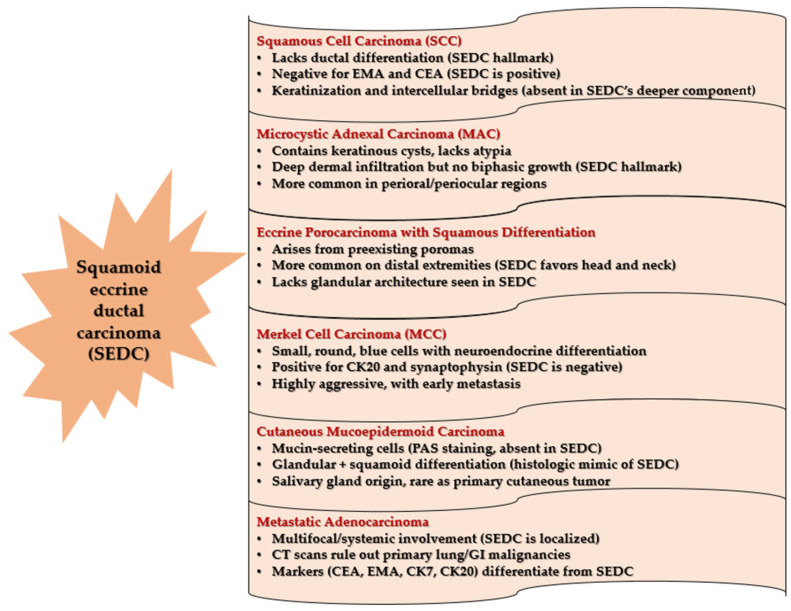
Background: Squamoid eccrine ductal carcinoma (SEDC) is an exceedingly rare and aggressive cutaneous adnexal malignancy, with fewer than 100 reported cases. Its histopathologic overlap with squamous cell carcinoma (SCC) frequently leads to misdiagnosis, delaying appropriate management. Unlike SCC, SEDC exhibits biphasic differentiation, deep infiltration, and a high rate of perineural invasion, contributing to significant morbidity and poor long-term outcomes. Given the absence of standardized treatment protocols, managing SEDC remains a challenge. Case Presentation: We report an unusual case of an 80-year-old female presenting with progressive numbness, nasal deviation, and a subcutaneous indurated lesion in the left nasofacial region. The early neurological symptoms were an atypical feature, suggesting perineural invasion (PNI) before visible tumor progression. Initial histopathologic evaluation was inconclusive, raising suspicion of SCC, necessitating immunohistochemical analysis, which confirmed ductal differentiation, leading to the final diagnosis of SEDC. The patient underwent radical resection with intraoperative margin assessment (Mohs micrographic surgery; MMS) followed by adjuvant radiotherapy (62 Gy/31 fractions) due to high-risk features, including perineural and perivascular invasion. Despite initial disease control, a local recurrence involving the left orbit and nasal bone occurred 20 months postoperatively, demonstrating the aggressive nature of SEDC despite clear surgical margins and adjuvant therapy. Due to disease progression and refusal of further surgery, only palliative care was provided. During follow-up, the patient contracted COVID-19, further complicating her clinical status and contributing to her demise. While COVID-19 was not directly linked to SEDC progression, its impact on patient management was significant. Conclusions: This case underscores the diagnostic and therapeutic challenges of SEDC, emphasizing the need for early suspicion, extensive histopathologic assessment, and aggressive multimodal treatment. The importance of multidisciplinary management-particularly in elderly and immunocompromised patients-and long-term surveillance due to high recurrence risk and PNI is crucial.
Keywords: Mohs micrographic surgery; adjuvant radiotherapy; aggressive skin neoplasm; cutaneous adnexal tumor; perineural invasion; squamoid eccrine ductal carcinoma.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Wick M.R., Swanson P.E. A Guide to Pathological Diagnosis. American Society of Clinical Pathologists; Chicago, IL, USA: 1991. Cutaneous Adnexal Tumors; pp. 10–13.
-
- Wong T.Y., Suster S., Mihm M.C. Squamoid Eccrine Ductal Carcinoma. Histopathology. 1997;30:288–293. - PubMed
-
- Brenn T. Malignant Sweat Gland Tumors: An Update. Adv. Anat. Pathol. 2015;22:242–253. - PubMed
-
- van der Horst M.P., Garcia-Herrera A., Markiewicz D., Martin B., Calonje E., Brenn T. Squamoid Eccrine Ductal Carcinoma: A Clinicopathologic Study of 30 Cases. Am. J. Surg. Pathol. 2016;40:755–760. - PubMed
-
- Bayramoğlu Z., Ünal B. Squamoid Eccrine Ductal Carcinoma: A Rare Case Report. Eur. Res. J. 2020;6:173–177. doi: 10.18621/eurj.502357. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
