

Effects of Physical Exercise on Walking Distance and Functional Limitations in Patients with Chronic Dyspnea
- PMID: 40282927
- PMCID: PMC12028406
- DOI: 10.3390/medicina61040636
Effects of Physical Exercise on Walking Distance and Functional Limitations in Patients with Chronic Dyspnea
Abstract
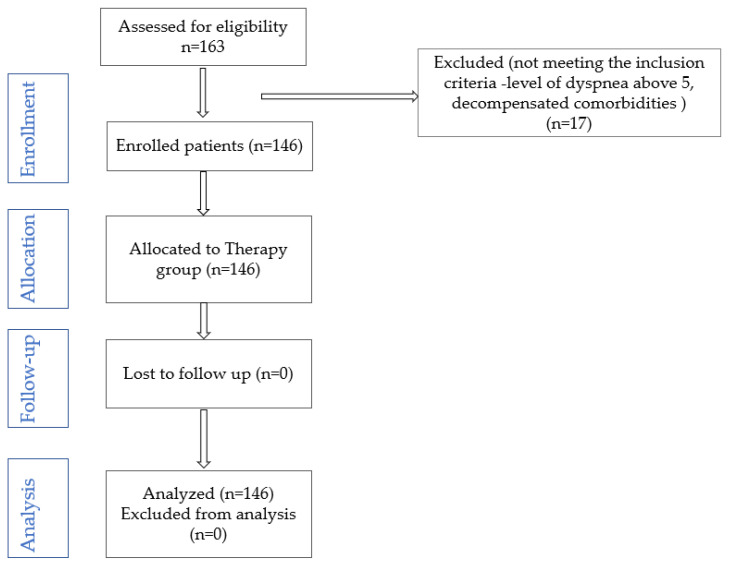
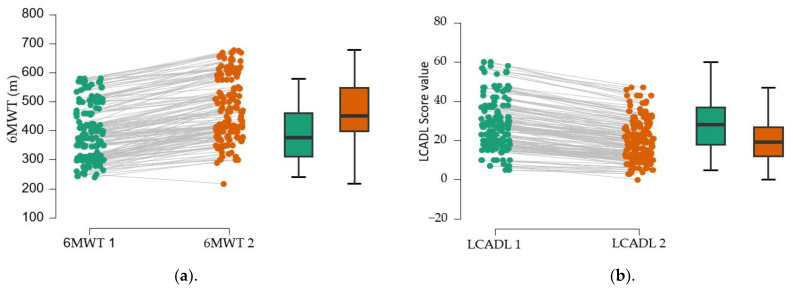
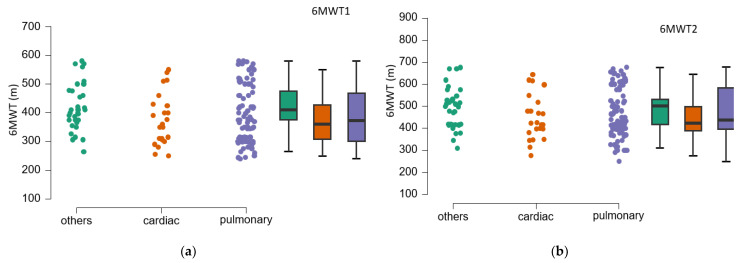
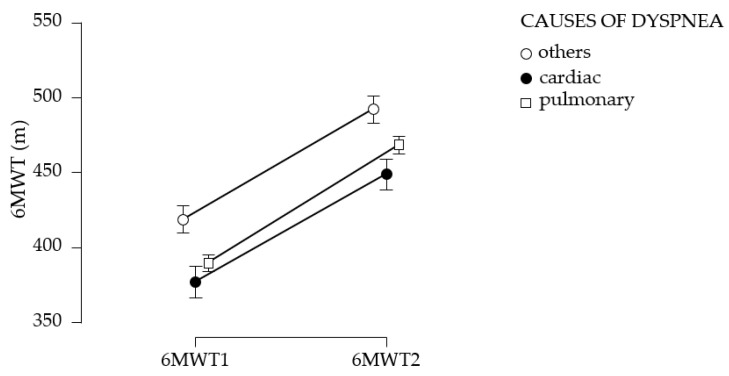
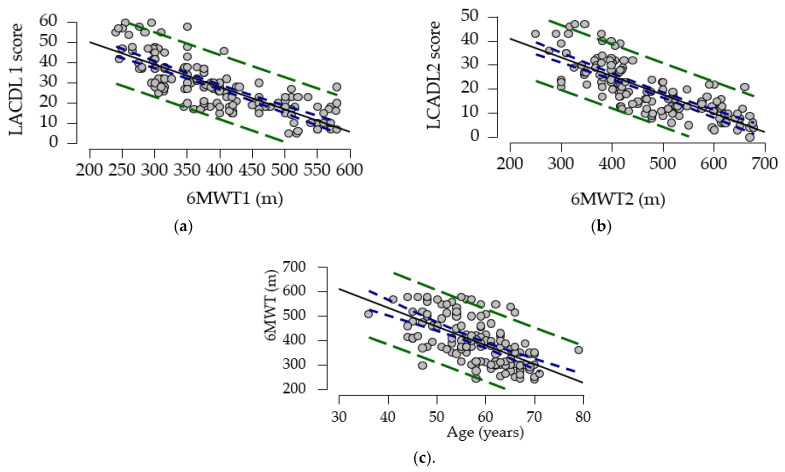
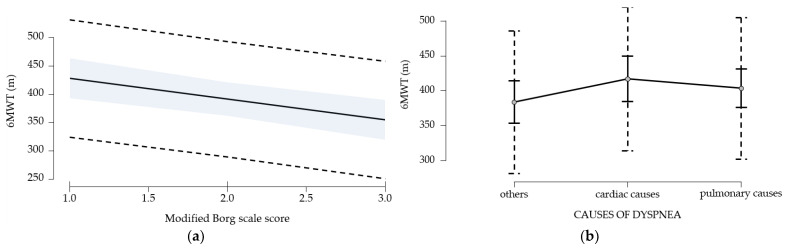
Background and Objectives: Chronic dyspnea is a common clinical manifestation in patients suffering from cardiovascular and respiratory diseases globally, representing an independent predictor of mortality for these patients. In addition, it may be a symptom associated with other conditions such as anemia, physical deconditioning, or anxiety. Methods: A prospective study was conducted, between 1 January 2021 and 30 June 2022, at the Medical Recovery Section from "Dr. Pop Mircea Municipal Hospital Pop Mircea" in Marghita. A total of 163 consecutive patients with chronic dyspnea of various etiologies were evaluated for inclusion in the study. Patients who met the inclusion criteria followed a personalized physical training program of variable duration (between 20 and 40 min) up to the limit of exercise tolerance (grade 3-4 modified Borg scale or up to 70% of maximum heart rate, calculated with the formula 220 age in years); the first 10 days, the training was supervised by a physiotherapist, then patients followed a program of 30 min of exercise 5 days/week at home for 3 months. Assessments, performed at inclusion and after 3 months of training, consisted of the 6 min walk test (6MWT) and the London Chest Activity of Daily Living (LCADL) scale. Results: Pulmonary etiology is the most common cause of dyspnea in the cohort (61.65%). The number of patients without ventilatory defects is 56, or 38.35%. The mean value of initial functional limitation (LCADL1) improved significantly after 3 months (LACDL2) of rehabilitation treatment (38% versus 26.5%); at the same time, the mean walking distance (6MWT) increased by 76 m. Conclusions: An adequate rehabilitation program and sedentary lifestyle change significantly reduce the functional limitation of the patient with chronic dyspnea and increase walking distance. Predictors for 6MWT gait test are age, LCADL score, dyspnea level, and cardiac etiology of chronic dyspnea.
Keywords: chronic dyspnea; functional limitation; physical workout; walking distance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Vindis K., Iovanovici D.C., Morenci M., Vasca E.M., Delia Nistor C.C., Pop M.S., Nemeth N., Bustea C., Tarce A.G., Babeș K., et al. The general essential objectives of medical rehabilitation in the management of chronic dyspnea—A systematic review. Balneo PRM Res. J. 2023;14:586. doi: 10.12680/balneo.2023.586. - DOI
-
- Wahls S.A. Causes and evaluation of chronic dyspnea. Am. Fam. Physician. 2012;86:173–182. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
