

A Retrospective Cohort Study on the Side Effects of Intrathecal Morphine Administration Combined with General Anaesthesia Versus General Anaesthesia Alone in Prostatectomy Patients
- PMID: 40283023
- PMCID: PMC12028477
- DOI: 10.3390/medicina61040732
A Retrospective Cohort Study on the Side Effects of Intrathecal Morphine Administration Combined with General Anaesthesia Versus General Anaesthesia Alone in Prostatectomy Patients
Abstract
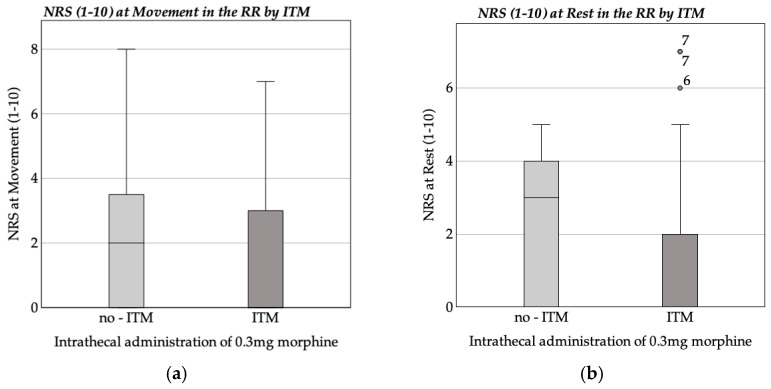
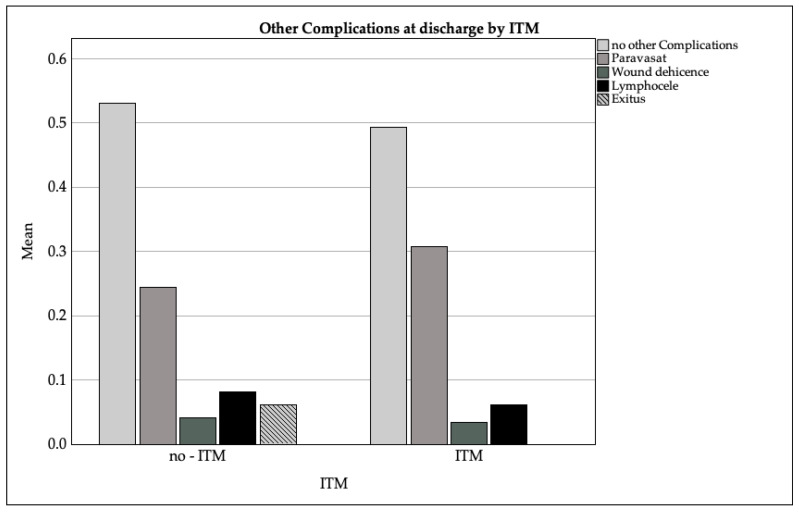
Background and Objectives: Prostatectomy is a common surgical procedure for prostate cancer, the most frequently diagnosed cancer in the male population. The choice of anaesthetic technique has a significant impact on postoperative pain management. The changes in recommendations between 2015 and 2021 prompted this study to evaluate the impact of intrathecal morphine administration in combination with general anaesthesia compared to general anaesthesia alone on postoperative analgesic consumption and the associated side effects. Material and Methods: A single-centre retrospective cohort study was conducted, analysing data from 202 patients who underwent a prostatectomy between 2015 and 2021. Patients were divided into two groups: 147 patients received intrathecal morphine combined with general anaesthesia, while 49 patients received general anaesthesia alone. Key postoperative parameters, including numerical rating scale (NRS) scores, analgesic consumption, and side effects (e.g., nausea, pruritus, hypotension, and respiratory depression) were evaluated. Statistical analyses were performed using Mann-Whitney U-tests and multiple regression models. Results: The group receiving intrathecal morphine showed a significant decrease in NRS pain scores at rest and during movement in the recovery room (p < 0.001). The need for postoperative analgesics, especially opioids such as piritramide, was reduced in this group. No significant increase in serious side effects such as respiratory depression was observed. Conclusions: The present study investigates the potential of intrathecal morphine combined with general anaesthesia as a promising approach to improve pain management in prostatectomy patients. By reducing pain intensity, this method shows significant clinical benefits. In addition, the absence of a significant increase in serious adverse events reinforces the safety of this approach. However, further studies are warranted to assess the long-term outcomes and explore optimal dosing strategies. The reintroduction of this anaesthetic technique has great potential to improve patient recovery and satisfaction following major surgery.
Keywords: analgesic consumption; general anaesthesia; intrathecal morphine; numerical rating scale (NRS); pain management; postoperative pain; prostatectomy; retrospective cohort study; side effects; spinal anaesthesia.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Alenezi B., Alsubhi M.H., Jin X., He G., Wei Q., Ke Y. Global Development on Causes, Epidemiology, Aetiology, and Risk Factors of Prostate Cancer: An Advanced Study. Highlights Med. Med. Sci. 2021;17:94–117.
-
- Mottet N., Cornford P., Briers E., Santis M.D., Gillessen S., Grummet J., Henry A.M. Eau-Eanm-Estro-Esur-Isup-Siog Guidelines on Prostate Cancer. European Association of Urology; Arnhem, The Netherlands: 2023. pp. 17–21+55–61+85.
-
- Groeben C., Koch R., Baunacke M., Flegar L., Borkowetz A., Thomas C., Huber J. Entwicklung Der Operativen Uroonkologie in Deutschland—Vergleichende Analysen Aus Populationsbasierten DatenTrends in Uro-Oncological Surgery in Germany—Comparative Analyses from Population-Based Data. Urologe. 2021;60:1257–1268. doi: 10.1007/s00120-021-01623-4. - DOI - PMC - PubMed
-
- Mottet N., van den Bergh R.C.N., Briers E., Van den Broeck T., Cumberbatch M.G., De Santis M., Fanti S., Fossati N., Gandaglia G., Gillessen S., et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021;79:243–262. doi: 10.1016/j.eururo.2020.09.042. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
