

Prevalence and Prognostic Significance of Chloride Levels in Patients with Acute Medical Conditions: A Prospective Observational Study
- PMID: 40283229
- PMCID: PMC12029041
- DOI: 10.3390/life15040676
Prevalence and Prognostic Significance of Chloride Levels in Patients with Acute Medical Conditions: A Prospective Observational Study
Abstract
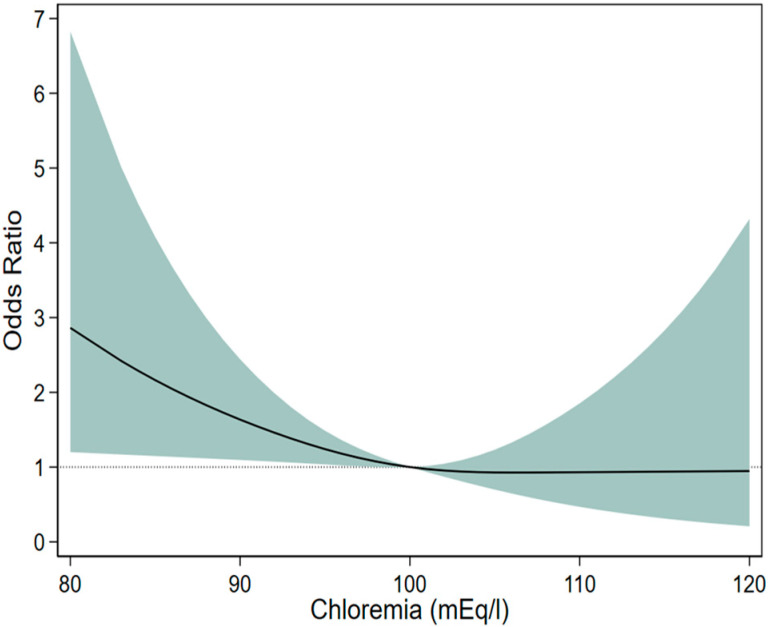
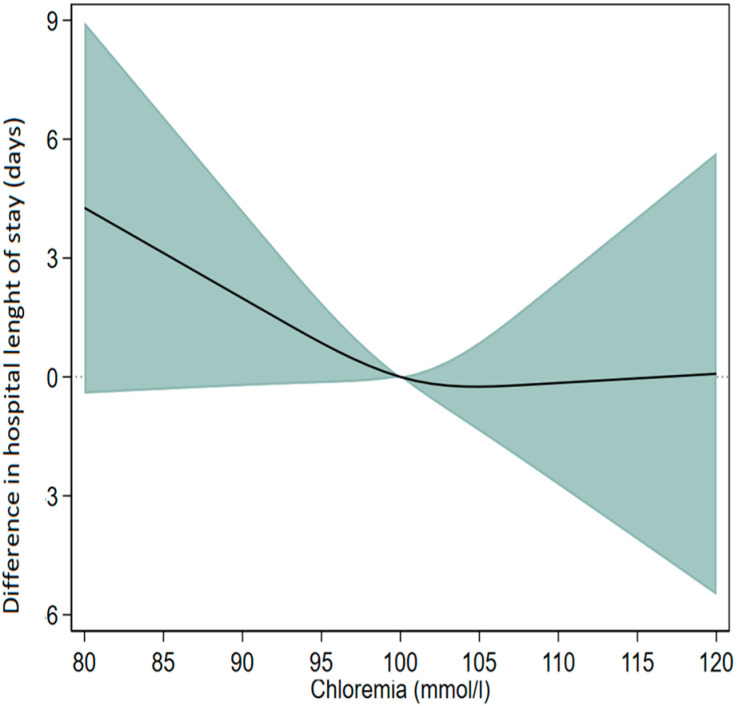
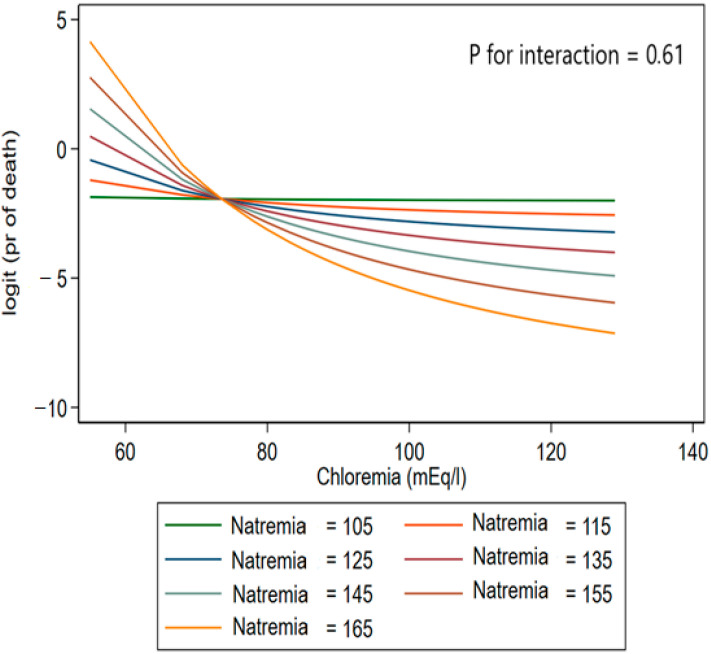
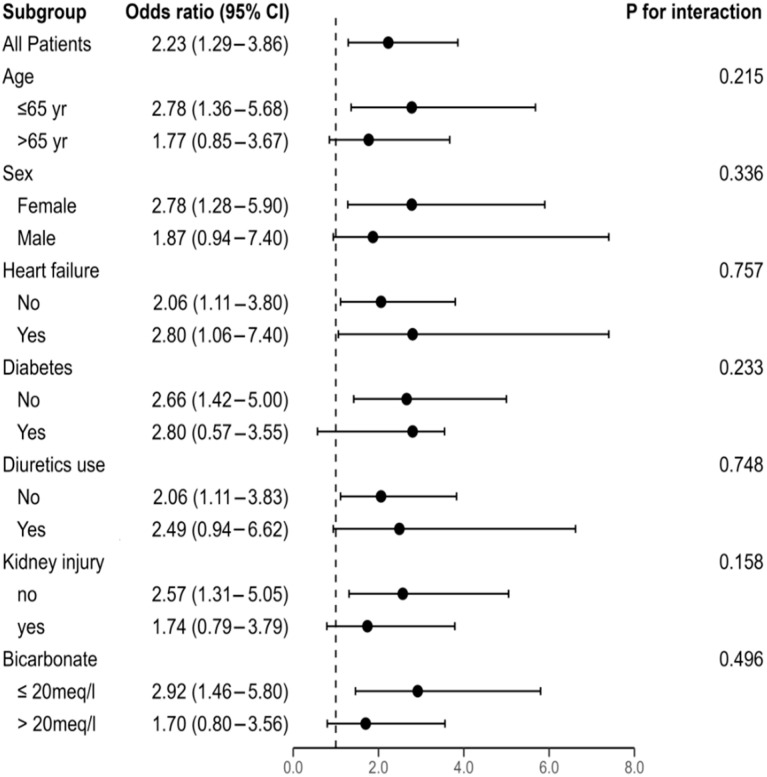
Chloride plays a considerable role in physiology. This study aimed to assess the association between serum chloride and prognosis in the population of adults with acute medical conditions. A prospective cohort study was conducted in an acute medical unit. Chloride levels at admission were the main exposure factor, categorized into hypochloremia, normochloremia, and hyperchloremia. The outcomes were in-hospital mortality and length of hospital stay (LOHS). A total of 798 patients were included. The mean age was 57.3 ± 18.3 years. The prevalence of dyschloremia was 40.9%. Restricted cubic splines revealed a linear association between hypochloremia and in-hospital mortality, as well as between hypochloremia and LOHS. After adjusting for age, sex, heart failure, diabetes, sodium, bicarbonates, creatinine, and diuretic use, hypochloremia was significantly associated with in-hospital mortality (OR = 2.23; 95% CI: 1.29, 3.86, p = 0.006), but not hyperchloremia (p = 0.57). Similarly, it was associated with a longer LOHS (β = 2.19; 95% CI: 0.01, 4.39, p = 0.05), but not hyperchloremia (p = 0.8). The interaction between chloride and sodium levels was not significant (p = 0.61). Subgroup analysis showed that the effect of hypochloremia on in-hospital mortality was consistent across subgroups. The prevalence of dyschloremia in this study was high at 40.9%. Hypochloremia increased the risk of in-hospital mortality and extended the LOHS. Differentiating the effects of chloride levels from those of sodium can enhance clinical risk stratification and enable a more targeted management approach for acutely ill patients. Recognizing this distinction is essential for optimizing prognostic assessment and tailoring treatment strategies accordingly.
Keywords: chloride; prevalence; prognosis; prospective observational study.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Hospital-Acquired Serum Chloride Derangements and Associated In-Hospital Mortality.Medicines (Basel). 2020 Jun 29;7(7):38. doi: 10.3390/medicines7070038. Medicines (Basel). 2020. PMID: 32610534 Free PMC article.
-
Association of Preoperative Serum Chloride Levels With Mortality and Morbidity After Noncardiac Surgery: A Retrospective Cohort Study.Anesth Analg. 2019 Dec;129(6):1494-1501. doi: 10.1213/ANE.0000000000003958. Anesth Analg. 2019. PMID: 31743168
-
Dyschloremia and Renal Outcomes in Critically Ill Patients With Sepsis: A Prospective Cohort Study: Dyschloremia and Renal Outcomes in Sepsis.Crit Care Res Pract. 2024 Oct 1;2024:8848405. doi: 10.1155/2024/8848405. eCollection 2024. Crit Care Res Pract. 2024. PMID: 39473920 Free PMC article.
-
U-Shaped Relationship of Sodium-to-chloride Ratio on admission and Mortality in Elderly Patients with Heart Failure: A Retrospective Cohort Study.Curr Probl Cardiol. 2023 Jan;48(1):101419. doi: 10.1016/j.cpcardiol.2022.101419. Epub 2022 Sep 28. Curr Probl Cardiol. 2023. PMID: 36181785 Review.
-
Chloride in intensive care units: a key electrolyte.F1000Res. 2017 Nov 1;6:1930. doi: 10.12688/f1000research.11401.1. eCollection 2017. F1000Res. 2017. PMID: 29123653 Free PMC article. Review.
Cited by
-
Initial serum chloride is associated with all-cause mortality in critically ill patients with acute kidney injury.Ren Fail. 2025 Dec;47(1):2536731. doi: 10.1080/0886022X.2025.2536731. Epub 2025 Jul 23. Ren Fail. 2025. PMID: 40697042 Free PMC article.
References
-
- Kondo T., Yamada T., Tamaki S., Morita T., Furukawa Y., Iwasaki Y., Kawasaki M., Kikuchi A., Ozaki T., Sato Y., et al. Serial Change in Serum Chloride During Hospitalization Could Predict Heart Failure Death in Acute Decompensated Heart Failure Patients. Circ. J. 2018;82:1041–1050. doi: 10.1253/circj.CJ-17-0938. - DOI - PubMed
LinkOut - more resources
Full Text Sources
