

Morphometric Measurements Prior to Totally Endoscopic Mitral Valve Repair: Technical and Educational Aspects
- PMID: 40283409
- PMCID: PMC12027974
- DOI: 10.3390/jcm14082581
Morphometric Measurements Prior to Totally Endoscopic Mitral Valve Repair: Technical and Educational Aspects
Abstract
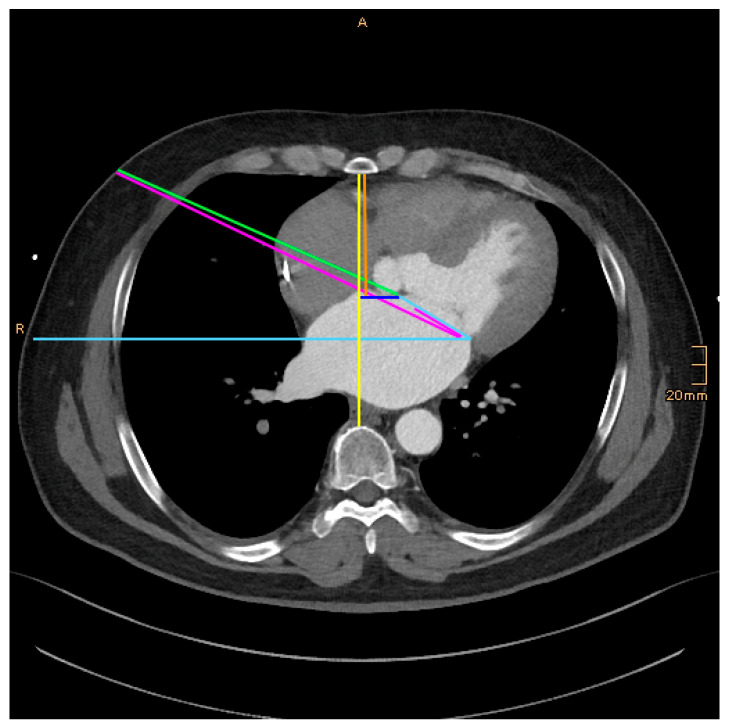
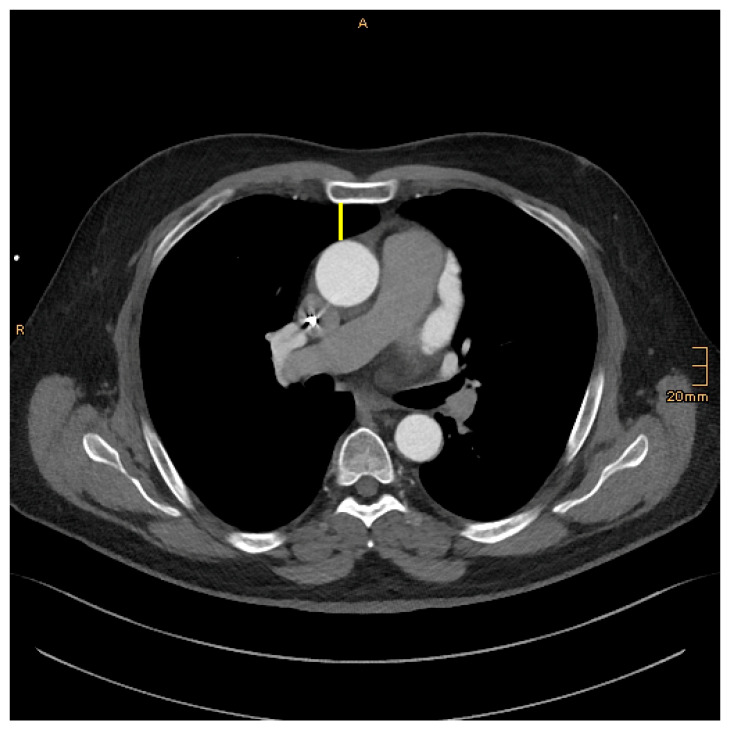
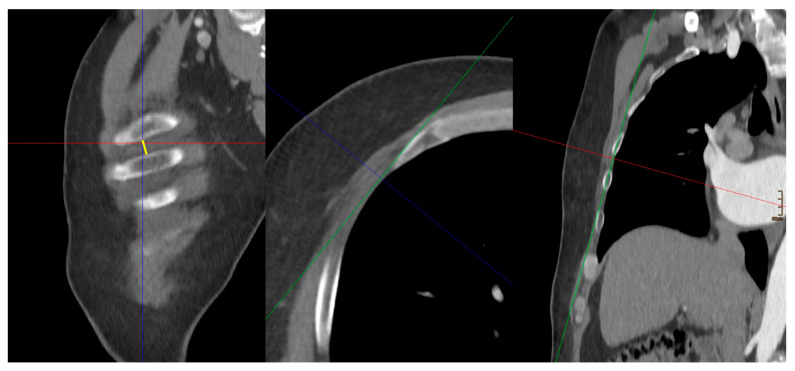
Objective: The totally endoscopic approach is on the rise to become the new standard in mitral valve surgery. The aim of this study was to develop a morphometric measurement tool for educational purposes to predict operability with low conversion and high repair rates. Methods: From January 2020 to March 2023, 64 patients underwent totally endoscopic mitral valve repair (TE-MVR). Of these, 15 patients were deemed to be unsuitable for TE-MVR due to narrow space and/or anticipated complex repair techniques and underwent repair through sternotomy (MVR-open). Angio-CT scanning was performed for preoperative planning and measurements of the following: the distance between the sternum and the spine (DSS), the distance between the skin incision and the anterior anulus of the mitral valve (DNM) and the intercostal space at the level of the skin incision (ICS). Results: The repair rate for all patients was 98.7%. In the TE-MVR group, the conversion rate to sternotomy was 3.1%. The 30-day survival was 100%. The DSS was 130.4 ± 18.8 mm and 108.1 ± 17.3 mm, and the DSM 70.7 ± 12.1 mm and 58.5 ± 13.6 mm in the TE-MVR and MVR-open, respectively (p < 0.001). Twenty-one TE-MVR patients were found to be technically demanding due to friction and less freedom to move the instruments. The composite morphometric parameter DSS plus 4xICS minus DNM was 53.3, 39.8 and 25.6 for TE-TMReasy, TE-TMRdemanding and MVR-open, respectively (p < 0.05 and p < 0.01). Conclusions: Surgical skills and a long history of expertise are mandatory to achieve excellent results with a low conversion and high repair rate. The composite morphometric parameter may be an easy tool for educational demands to predict the ease and feasibility of TE-MVR.
Keywords: computed tomography; minimally invasive; mitral valve repair; totally endoscopic.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Stelzmueller M.-E., Zilberszac R., Rosenhek R., Hutschala D., Kappel S., Lassnig A., Laufer G., Zimpfer D., Wisser W. Pushing boundaries in cardiac surgery: Minimally invasive mitral valve repair combined with tricuspid valve repair and/or other concomitant procedures. Front. Cardiovasc. Med. 2024;11:1407591. doi: 10.3389/fcvm.2024.1407591. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
