

Management of Hemodynamic and Respiratory Instability and Anesthetic Approaches in Patients Undergoing Pulmonary Thrombectomy for Pulmonary Embolism
- PMID: 40283535
- PMCID: PMC12028100
- DOI: 10.3390/jcm14082704
Management of Hemodynamic and Respiratory Instability and Anesthetic Approaches in Patients Undergoing Pulmonary Thrombectomy for Pulmonary Embolism
Abstract
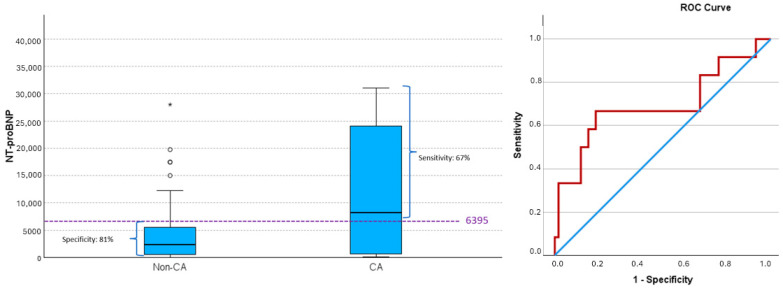
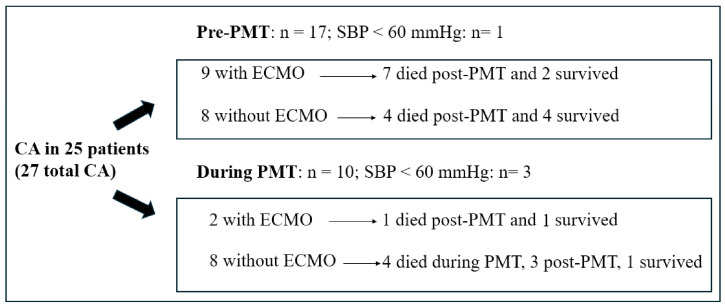
Background/Objectives: The incidence, timing, and predictors of hemodynamic and respiratory deterioration in patients with high-risk or intermediate-high-risk pulmonary embolism (PE) undergoing pulmonary mechanical thrombectomy (PMT) remain poorly understood. This hemodynamic and respiratory instability can lead to modifications in the anesthetic management. This study investigates these key factors and quantifies the 30-day mortality following thrombectomy. Methods: A retrospective study was conducted on 98 patients aged ≥18 years who underwent PMT. Patients were categorized based on the occurrence of cardiac arrest (CA). Results: Of the 98 patients, 34 had high-risk PE, 62 intermediate/high-risk, and 2 low risk. There were 27 cases of CA, 17 pre- and 10 intra-PMT. An SBP < 90 mmHg increases the risk of CA by 33 (p < 0.001); men have an 8-fold higher risk than women (p = 0.004); SpO2 <90% by 6 (p = 0.012); and pre-existing respiratory conditions increase the risk by 4 (p = 0.047)). N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels were 8206 ± 11660.86 and 2388.50 ± 5683.71 pg/mL (p = 0.035) in patients with and without CA, respectively. During PMT, 14% of patients required increased vasoactive drug use, and 38.77% were intubated, including 12 who required ECMO support. Sedation was administered in 64.3% of patients, while general anesthesia was used in 38.8%, with a preemptive indication in 23.5%. The survival rate of patients without CA before and/or during PMT was 96%. Conclusions: While PMT was successfully performed in all patients, hemodynamic and respiratory instability remained a significant concern. More than 10% of patients experienced severe hemodynamic instability, primarily during thrombus extraction, requiring conversion from sedation to general anesthesia. Male sex, pre-existing respiratory disease, SpO2 < 90%, and SBP < 90 mmHg were associated with an increased risk of CA. Additionally, elevated NT-proBNP levels were linked to a higher incidence of CA.
Keywords: cardiorespiratory arrest; hemodynamic instability; hypotension; pulmonary embolism; pulmonary mechanical thrombectomy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Rivera-Lebron B., McDaniel M., Ahrar K., Alrifai A., Dudzinski D.M., Fanola C., Blais D., Janicke D., Melamed R., Mohrien K., et al. Diagnosis, treatment and follow up of acute pulmonary embolism: Consensus practice from the pert consortium. Clin. Appl. Thromb. Hemost. 2019;25:1076029619853037. doi: 10.1177/1076029619853037. - DOI - PMC - PubMed
-
- Giri J., Sista A.K., Weinberg I., Kearon C., Kumbhani D.J., Desai N.D., Piazza G., Gladwin M.T., Chatterjee S., Kobayashi T., et al. Interventional Therapies for acute pulmonary embolism: Current status and principles for the development of novel evidence: A scientific statement from the American Heart Association. Circulation. 2019;140:E774–E801. doi: 10.1161/CIR.0000000000000707. - DOI - PubMed
-
- Konstantinides S.V., Meyer G., Becattini C., Bueno H., Geersing G.J., Harjola V.-P., Huisman M.V., Humbert M., Jennings C.S., Jiménez D., et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur. Heart J. 2020;41:543–603. doi: 10.1093/eurheartj/ehz405. - DOI - PubMed
-
- Tu T., Toma C., Tapson V.F., Adams C., Jaber W.A., Silver M., Khandhar S., Amin R., Weinberg M., Engelhardt T., et al. A prospective, single-arm, multicenter trial of catheter-directed mechanical thrombectomy for intermediate-riskacute pulmonary embolism: The FLARE study. J. Am. Coll. Cardiovasc. Interv. 2019;12:859–869. doi: 10.1016/j.jcin.2018.12.022. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
