

Investigating Peri-Ictal MRI Abnormalities: A Prospective Neuroimaging Study on Status Epilepticus, Seizure Clusters, and Single Seizures
- PMID: 40283540
- PMCID: PMC12028061
- DOI: 10.3390/jcm14082711
Investigating Peri-Ictal MRI Abnormalities: A Prospective Neuroimaging Study on Status Epilepticus, Seizure Clusters, and Single Seizures
Abstract
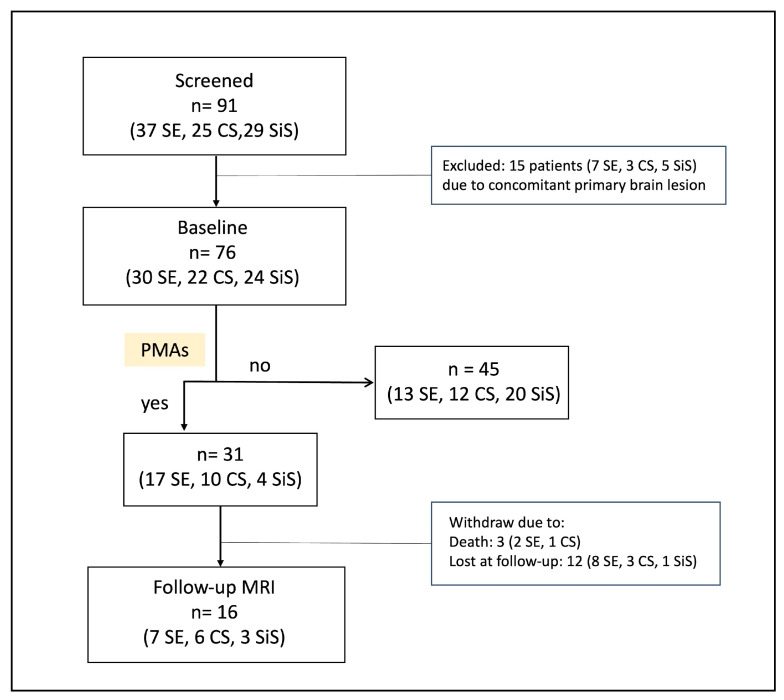
Background/Objectives: Brain magnetic resonance imaging (MRI) often reveals acute peri-ictal abnormalities (PMAs) during or shortly after status epilepticus (SE) but also following single seizures (SiS) or clusters of seizures (CS). However, the incidence, characteristics, and progression remain not clearly known. This study aimed to investigate incidence, clinical correlations, and evolution of PMAs in SE, CS, and SiS patients. Methods: This prospective observational study enrolled patients with SE, CS, and SiS who underwent MRI within 120 h of the ictal event. Demographic, clinical, EEG, and MRI data were collected. Patients with PMAs (PMAs+) underwent serial follow-up MRI. Incidence, association with clinical characteristics, and progression of PMAs were analyzed across the three groups. Results: Among 76 patients (30 SE, 22 CS, 24 SiS), PMAs were observed in 31 (41%), with a significant difference between groups (p = 0.011), as PMAs were less frequent in SiS (17%) compared to SE (57%) and CS (45%) patients. Acute symptomatic SE/seizures were significantly more common in PMAs+ compared to PMAs- in the overall cohort (52% vs. 29%; p = 0.045) and in the SiS group (100% vs. 25%; p = 0.031). History of epilepsy was less frequent in PMAs+ in the whole cohort (13% vs. 40%; p = 0.011) and in SE in particular (12% vs. 46%, p = 0.049). No association between PMAs and seizure type, SE duration, etiology, time to MRI, and EEG findings (p > 0.005) was found. The temporal cortex and hippocampus were most frequently affected by PMAs. Follow-up MRI performed in 16 patients showed resolution of PMAs in 75% (5/7 SE, 3/6 CS, 3/3 SiS) within a median time of 24 days (IQR: 8-39). Conclusions: PMAs were more common in SE and CS than in SiS. Acute underlying pathology was frequently associated with PMAs. While duration of ictal activity is an important factor, it was not the sole determinant. Most PMAs resolved, particularly in SiS. Further studies are needed to clarify the pathophysiological mechanism and clinical implications of PMAs.
Keywords: convulsive status epilepticus; epilepsy; non-convulsive status epilepticus; peri-ictal DWI abnormalities; peri-ictal FLAIR abnormalities; transient MRI hyperintensity.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Bauer G., Gotwald T., Dobesberger J., Embacher N., Felber S., Bauer R., Seppi K., Walser G., Trinka E., Poewe W. Transient and permanent magnetic resonance imaging abnormalities after complex partial status epilepticus. Epilepsy Behav. 2006;8:666–671. doi: 10.1016/j.yebeh.2006.01.002. - DOI - PubMed
LinkOut - more resources
Full Text Sources
