

Spinal Drainage and Combined Pharmacotherapy as Potential Strategies to Improve Outcomes for Patients with Poor-Grade Subarachnoid Hemorrhage Treated with Clipping or Coiling but Not Receiving Nimodipine
- PMID: 40283546
- PMCID: PMC12027632
- DOI: 10.3390/jcm14082715
Spinal Drainage and Combined Pharmacotherapy as Potential Strategies to Improve Outcomes for Patients with Poor-Grade Subarachnoid Hemorrhage Treated with Clipping or Coiling but Not Receiving Nimodipine
Abstract
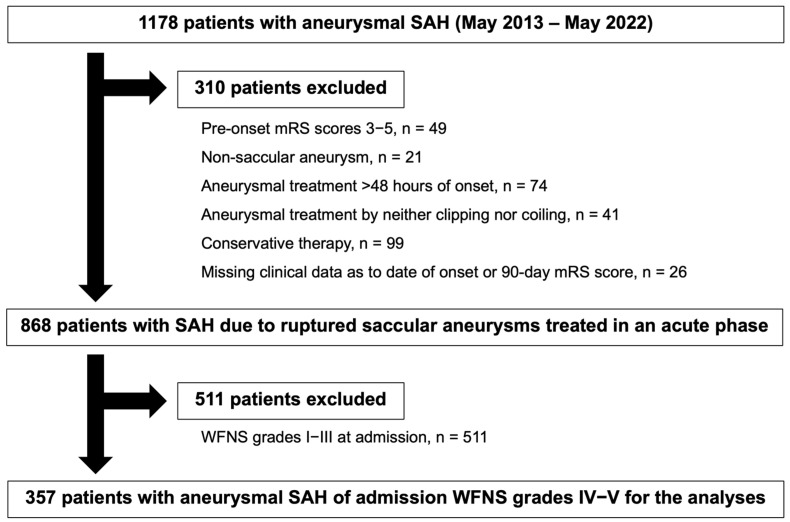
Background/Objectives: The outcome for aneurysmal subarachnoid hemorrhage (SAH) remains poor, particularly for patients presenting with World Federation of Neurological Surgeons (WFNS) grades IV-V. This study was designed to identify independent prognostic factors in this group of patients with poor-grade SAH. Methods: We prospectively analyzed 357 SAH patients with admission WFNS grades IV-V enrolled in nine primary stroke centers in Mie prefecture, Japan, from 2013 to 2022. This study compared clinical variables, including treatments for angiographic vasospasm and delayed cerebral ischemia (DCI), between patients with favorable (modified Rankin Scale [mRS] scores 0-2) and unfavorable (mRS scores 3-6) outcomes at 90 days post-onset. Multivariate analyses were then performed to identify independent determinants of favorable 90-day outcomes, followed by propensity score matching analyses. Results: The median age was 68 years, and 53.5% of patients had admission WFNS grade V. DCI occurred in 12.9% of patients, and 66.9% had unfavorable outcomes. Independent variables related to unfavorable outcomes were older age, admission WFNS grade V, ventricular drainage, edaravone administration, and delayed cerebral infarction, while those for favorable outcomes were spinal drainage (adjusted odds ratio [aOR] 6.118, 95% confidence interval [CI] 2.687-13.927, p < 0.001), modified Fisher grade 3 (aOR 2.929, 95% CI 1.668-5.143, p < 0.001), and triple prophylactic anti-DCI medication consisting of cilostazol, fasudil hydrochloride and eicosapentaenoic acid (aOR 1.869, 95% CI 1.065-3.279, p = 0.029). Nimodipine is not approved in Japan, and statin and cerebral vasospasm did not influence outcomes. As spinal drainage and the triple prophylactic anti-DCI medication were intervenable variables, propensity score matchings were performed, and they confirmed that both spinal drainage and the triple prophylactic anti-DCI medication were useful to achieve favorable outcomes. Conclusions: In poor-grade SAH, spinal drainage and the triple prophylactic anti-DCI medication may be effective in improving outcomes, possibly by suppressing DCI pathologies other than cerebral vasospasm.
Keywords: cerebral vasospasm; cerebrospinal fluid drainage; cilostazol; delayed cerebral ischemia; early brain injury; eicosapentaenoic acid; fasudil hydrochloride; outcome; subarachnoid hemorrhage.
Conflict of interest statement
Hidenori Suzuki reported personal fees from Eisai, Kowa, Otsuka, and Nxera Pharma, and a research fund from Japan Blood Products Organization and Nxera Pharma outside the submitted work. The other authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Cilostazol May Improve Outcomes Even in Patients with Aneurysmal Subarachnoid Hemorrhage Aged 75 Years and Older: Multicenter Cohort Study and Propensity Score-Matched Analyses.World Neurosurg. 2024 Jan;181:e273-e290. doi: 10.1016/j.wneu.2023.10.039. Epub 2023 Oct 13. World Neurosurg. 2024. PMID: 37839574
-
Outcome after Hunt and Hess Grade V subarachnoid hemorrhage: a comparison of pre-coiling era (1980-1995) versus post-ISAT era (2005-2014).J Neurosurg. 2018 Jan;128(1):100-110. doi: 10.3171/2016.8.JNS161075. Epub 2017 Feb 24. J Neurosurg. 2018. PMID: 28298025
-
Analysis of Angiographic Treatment Response to Intra-Arterial Nimodipine Bolus Injection in Patients with Medically Refractory Cerebral Vasospasm After Spontaneous Subarachnoid Hemorrhage.World Neurosurg. 2022 Jun;162:e457-e467. doi: 10.1016/j.wneu.2022.03.033. Epub 2022 Mar 12. World Neurosurg. 2022. PMID: 35292409
-
Effect of statin treatment on vasospasm-related morbidity and functional outcome in patients with aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2017 Aug;127(2):291-301. doi: 10.3171/2016.5.JNS152900. Epub 2016 Oct 7. J Neurosurg. 2017. PMID: 27715439
-
Clinical Burden of Angiographic Vasospasm and Its Complications After Aneurysmal Subarachnoid Hemorrhage: A Systematic Review.Neurol Ther. 2023 Apr;12(2):371-390. doi: 10.1007/s40120-022-00436-7. Epub 2023 Jan 7. Neurol Ther. 2023. PMID: 36609962 Free PMC article. Review.
References
-
- Scibilia A., Rustici A., Linari M., Zenesini C., Belotti L.M.B., Dall’Olio M., Princiotta C., Cuoci A., Aspide R., Migliorino E., et al. Factors affecting 30-day mortality in poor-grade aneurysmal subarachnoid hemorrhage: A 10-year single-center experience. Front. Neurol. 2024;15:1286862. doi: 10.3389/fneur.2024.1286862. - DOI - PMC - PubMed
-
- Hironaka K., Aso S., Suzuki M., Matano F., Matsui H., Fushimi K., Yasunaga H., Morita A. Outcomes in elderly Japanese patients treated for aneurysmal subarachnoid hemorrhage: A retrospective nationwide study. J. Stroke Cerebrovasc. Dis. 2020;29:104795. doi: 10.1016/j.jstrokecerebrovasdis.2020.104795. - DOI - PubMed
-
- Nakajima H., Kawakita F., Okada T., Oinaka H., Suzuki Y., Nampei M., Kitano Y., Nishikawa H., Fujimoto M., Miura Y., et al. Treatment factors to suppress delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage based on VASOGRADE: Multicenter cohort study. Neurosurg. Rev. 2024;47:564. doi: 10.1007/s10143-024-02795-1. - DOI - PubMed
-
- Lenkeit A., Oppong M.D., Dinger T.F., Gümüs M., Rauschenbach L., Chihi M., Ahmadipour Y., Uerschels A.K., Dammann P., Deuschl C., et al. Risk factors for poor outcome after aneurysmal subarachnoid hemorrhage in patients with initial favorable neurological status. Acta Neurochir. 2024;166:93. doi: 10.1007/s00701-024-05968-5. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
