

The Association Between Erythropoiesis Resistance Index and Clinical Outcomes in Hemodialysis Patients: A Nationwide Study
- PMID: 40283642
- PMCID: PMC12028047
- DOI: 10.3390/jcm14082812
The Association Between Erythropoiesis Resistance Index and Clinical Outcomes in Hemodialysis Patients: A Nationwide Study
Abstract
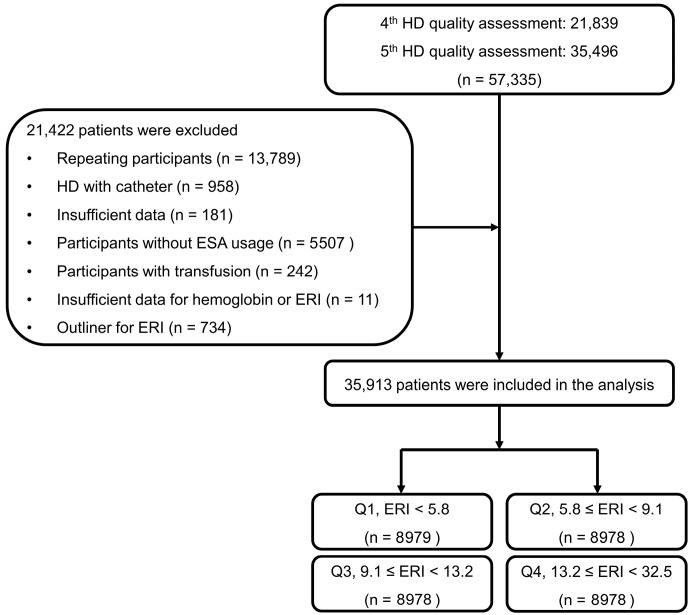
Background: Although erythropoiesis-stimulating agent (ESA) therapy is fundamental for correcting anemia, excessive ESA administration is associated with increased risks. This study aimed to investigate the impact of the erythropoietin resistance index (ERI) on clinical outcomes in a population-based cohort of hemodialysis (HD) patients. Methods: This retrospective study analyzed datasets from patients who underwent periodic HD quality assessments and their claims data. Overall, we included 35,913 patients. Participants were divided into quartiles based on the ERI during the 6-month assessment period: Q1, Q2, Q3, and Q4 groups. Results: The 5-year survival rates were 68.8% (Q1), 67.8% (Q2), 66.9% (Q3), and 60.2% (Q4) (p < 0.001). Multivariable analysis showed the same trends as the univariable analysis. Additionally, a spline curve using the multivariable model indicated that the increased ERI was linked to all-cause mortality. However, cardiovascular events were not associated with ERI quartiles in Cox regression analyses. Subgroup analysis revealed that in most subgroups, the all-cause mortality was significantly higher in those with a high ERI than in those with a low ERI. Further analysis using the balanced cohort, which attenuated baseline characteristic differences, confirmed that the high mortality in those with a high ERI was maintained. Conclusions: Our population-based cohort study reveals an association between the ERI and all-cause mortality in HD patients.
Keywords: erythropoiesis resistance; erythropoiesis-stimulating agent; hemodialysis; mortality.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures


Similar articles
-
Association between hyporesponsiveness to erythropoiesis-stimulating agents and risk of brain hemorrhage in patients undergoing hemodialysis: the Q-Cohort Study.Clin Exp Nephrol. 2023 Jan;27(1):79-88. doi: 10.1007/s10157-022-02278-x. Epub 2022 Sep 13. Clin Exp Nephrol. 2023. PMID: 36100804
-
Relationships among the Dosage of Erythropoiesis-Stimulating Agents, Erythropoietin Resistance Index, and Mortality in Maintenance Hemodialysis Patients.Blood Purif. 2022;51(2):171-181. doi: 10.1159/000506536. Epub 2021 Jun 25. Blood Purif. 2022. PMID: 34175850
-
Not baseline but time-dependent erythropoiesis-stimulating agent responsiveness predicts cardiovascular disease in hemodialysis patients receiving epoetin beta pegol: A multicenter prospective PARAMOUNT-HD Study.Int J Cardiol. 2023 Mar 15;375:110-118. doi: 10.1016/j.ijcard.2022.12.051. Epub 2022 Dec 30. Int J Cardiol. 2023. PMID: 36592827
-
Association of plasma F2-isoprostanes and isofurans concentrations with erythropoiesis-stimulating agent resistance in maintenance hemodialysis patients.BMC Nephrol. 2015 Jun 5;16:79. doi: 10.1186/s12882-015-0074-9. BMC Nephrol. 2015. PMID: 26045064 Free PMC article.
-
Butyrylcholinesterase level as an independent factor of erythropoiesis-stimulating agent resistance in patients on maintenance hemodialysis: a single-center cross-sectional study.Clin Exp Nephrol. 2018 Oct;22(5):1174-1181. doi: 10.1007/s10157-018-1569-z. Epub 2018 Mar 29. Clin Exp Nephrol. 2018. PMID: 29600410
References
-
- Kim K.M., Jeong S.A., Ban T.H., Hong Y.A., Hwang S.D., Choi S.R., Lee H., Kim J.H., Kim S.H., Kim T.H., et al. Status and trends in epidemiologic characteristics of diabetic end-stage renal disease: An analysis of the 2021 Korean Renal Data System. Kidney Res. Clin. Pract. 2024;43:20–32. doi: 10.23876/j.krcp.23.130. - DOI - PMC - PubMed
-
- KDIGO Anemia Work Group KDIGO Clinical Practice Guideline for Anemia in Chronic Kidney Disease. Kidney Int. Suppl. 2012;2:279–335.
Grants and funding
LinkOut - more resources
Full Text Sources
