

Transcatheter Aortic Valve Replacement Reverses Heyde Syndrome: A Case Report of Severe Aortic Stenosis and Gastrointestinal Bleeding
- PMID: 40283648
- PMCID: PMC12027620
- DOI: 10.3390/jcm14082819
Transcatheter Aortic Valve Replacement Reverses Heyde Syndrome: A Case Report of Severe Aortic Stenosis and Gastrointestinal Bleeding
Abstract
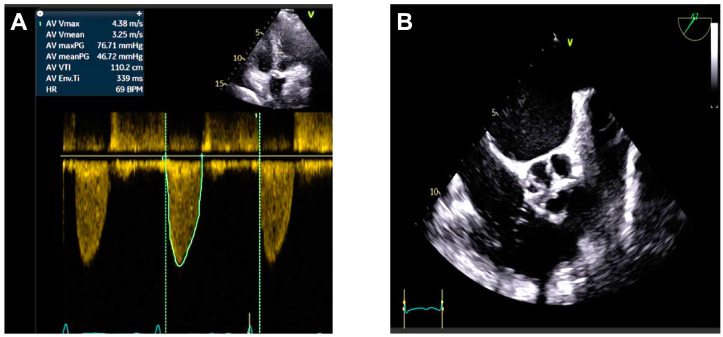
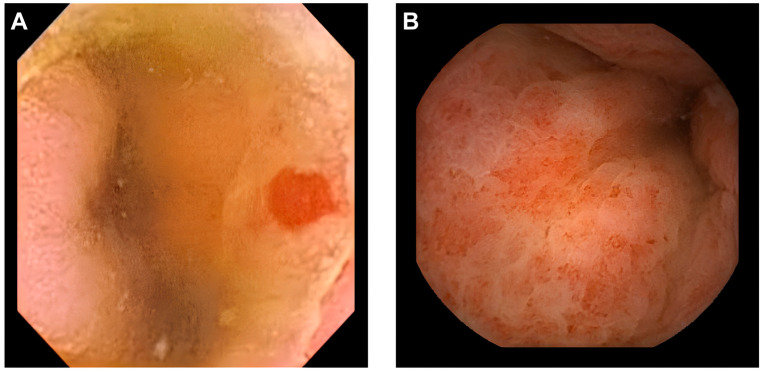
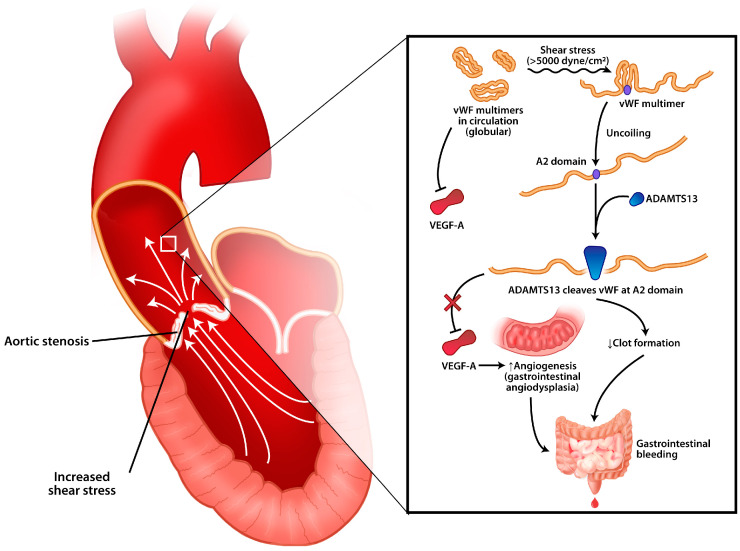
Background: Heyde syndrome is a rare condition characterized by the triad of severe aortic stenosis, gastrointestinal bleeding, and acquired type 2A von Willebrand syndrome. This case report highlights the diagnostic and therapeutic approach for a 72-year-old woman presenting with exertional chest pain, dyspnea, fatigue, and a history of melena. Methods: The diagnostic workup revealed severe microcytic anemia and a reduced vWF ristocetin-to-antigen ratio. Imaging confirmed severe degenerative aortic stenosis, while video capsule endoscopy identified angiodysplasia and telangiectasias in the small bowel as the source of gastrointestinal bleeding. Following evaluation by a multidisciplinary Heart Team, the patient underwent transcatheter aortic valve replacement (TAVR) with an Evolut Fx self-expanding prosthesis. Results: Post-procedural echocardiography showed mild paravalvular regurgitation. The patient's clinical course was favorable, with resolution of anemia and no further gastrointestinal bleeding episodes. Conclusions: Heyde syndrome requires a high index of suspicion for diagnosis in patients with severe aortic stenosis and unexplained anemia or gastrointestinal bleeding. TAVR offers an effective treatment option that not only resolves valvular pathology, but also mitigates associated bleeding risks.
Keywords: Heyde syndrome; acquired von Willebrand syndrome; angiodysplasia; aortic stenosis; gastrointestinal bleeding; transcatheter aortic valve replacement (TAVR); video capsule endoscopy (VCE); von Willebrand factor (vWF).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
Refractory Iron-Deficiency Anemia and Vascular Malformation Concomitant with Aortic Stenosis: Heyde Syndrome.Am J Case Rep. 2024 Sep 26;25:e944440. doi: 10.12659/AJCR.944440. Am J Case Rep. 2024. PMID: 39325680 Free PMC article.
-
Aortic Valve Replacement for the Management of Heyde Syndrome: A Case Report.J Nippon Med Sch. 2017;84(4):193-197. doi: 10.1272/jnms.84.193. J Nippon Med Sch. 2017. PMID: 28978901
-
von Willebrand Factor Abnormalities and Heyde Syndrome in Dysfunctional Heart Valve Prostheses.JAMA Cardiol. 2016 May 1;1(2):198-204. doi: 10.1001/jamacardio.2016.0075. JAMA Cardiol. 2016. PMID: 27437891
-
Effectiveness of aortic valve replacement in Heyde syndrome: a meta-analysis.Eur Heart J. 2023 Sep 1;44(33):3168-3177. doi: 10.1093/eurheartj/ehad340. Eur Heart J. 2023. PMID: 37555393 Free PMC article.
-
Aortic Valve Replacement for Patients with Heyde Syndrome: A Literature Review.Chin Med Sci J. 2021 Dec 31;36(4):307-315. doi: 10.24920/003881. Chin Med Sci J. 2021. PMID: 34986967 Review.
References
-
- Talanas G., Laconi A., Kereiakes D.J., Merella P., Reardon M.J., Spano A., Petretto G., Lauriola F., Casula M., Micheluzzi V., et al. Long-Term Outcomes of Transcatheter vs Surgical Aortic Valve Replacement: Meta-analysis of Randomized Trials. J. Soc. Cardiovasc. Angiogr. Interv. 2024;3:102143. doi: 10.1016/j.jscai.2024.102143. - DOI - PMC - PubMed
-
- Krishnapillai A., Omar M.A., Ariaratnam S., Awaluddin S., Sooryanarayana R., Kiau H.B., Tauhid N.M., Ghazali S.S. The Prevalence of Anemia and Its Associated Factors Among Older Persons: Findings from the National Health and Morbidity Survey (NHMS) 2015. Int. J. Environ. Res. Public Health. 2022;19:4983. doi: 10.3390/ijerph19094983. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
