

Using Physiologically Based Pharmacokinetic Models for Assessing Pharmacokinetic Drug-Drug Interactions in Patients with Chronic Heart Failure Taking Narrow Therapeutic Window Drugs
- PMID: 40283914
- PMCID: PMC12030730
- DOI: 10.3390/ph18040477
Using Physiologically Based Pharmacokinetic Models for Assessing Pharmacokinetic Drug-Drug Interactions in Patients with Chronic Heart Failure Taking Narrow Therapeutic Window Drugs
Abstract
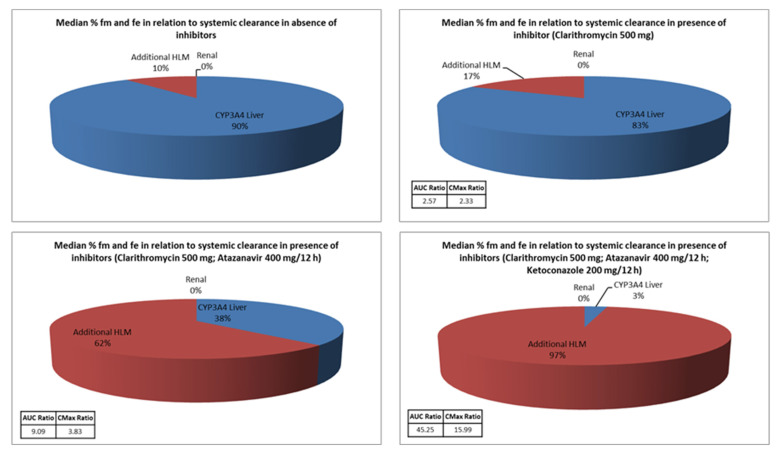
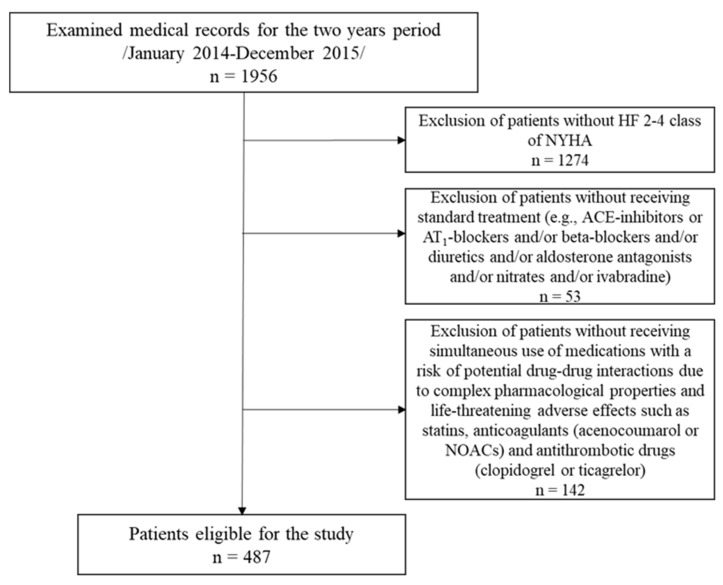
Background: Pharmacotherapy of chronic heart failure (CHF) with a reduced ejection fraction includes a combination of drugs. Often, different groups of drugs are added together for the treatment of concomitant conditions, such as statins, anticoagulants, antiplatelet agents, and cardiac glycosides, which have a narrow therapeutic window. Increased medication intake is a prerequisite for the increased risk of potential adverse drug-drug interactions (DDI), especially those occurring at the pharmacokinetic level. The main objectives of this study are to identify the most common potential pharmacokinetic drug-drug interactions (pPKDDIs), to explore more complex cases, and to simulate and analyze them with appropriate software. Methods: The data selected for the simulations were collected over a two-year period from January 2014 to December 2015. Identification of the pPKDDIs was carried out using Lexicomp Drug interaction, while simulations were performed with Simcyp software (V20, R1). Results: The most common pharmacokinetic mechanisms responsible for the occurrence of drug-drug interactions in the selected drugs with narrow therapeutic windows are those featuring the cytochrome isoforms CYP3A4 and 2C9 and the efflux pump-P-glycoprotein (P-gp). Simulations with the available data in Simcyp software showed possibilities to analyze and evaluate pPKDDIs, which would be difficult to assess without appropriate software, as well as ways to manage them. Conclusions: The frequency and complexity of pPKDDIs in patients with cardiovascular disease are high. Therefore, such patients require a specific approach to reduce these risks as well as to optimize the therapy. An appropriate PBPK software with the necessary database would be suitable in these cases.
Keywords: CYP2C9; CYP3A4; P-gp; physiologically based pharmacokinetic (PBPK) modeling; potential drug–drug interactions (pDDIs); potential pharmacokinetic drug–drug interactions (pPKDDIs).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Prevalence of polypharmacy and risk of potential drug-drug interactions among hospitalized patients with emphasis on the pharmacokinetics.Sci Prog. 2022 Jan-Mar;105(1):368504211070183. doi: 10.1177/00368504211070183. Sci Prog. 2022. PMID: 35072561 Free PMC article.
-
Drug-drug interaction (DDI) assessments of ruxolitinib, a dual substrate of CYP3A4 and CYP2C9, using a verified physiologically based pharmacokinetic (PBPK) model to support regulatory submissions.Drug Metab Pers Ther. 2019 May 30;34(2):/j/dmdi.2019.34.issue-2/dmpt-2018-0042/dmpt-2018-0042.xml. doi: 10.1515/dmpt-2018-0042. Drug Metab Pers Ther. 2019. PMID: 31145690
-
Physiologically Based Pharmacokinetic Modelling of Cytochrome P450 2C9-Related Tolbutamide Drug Interactions with Sulfaphenazole and Tasisulam.Eur J Drug Metab Pharmacokinet. 2018 Jun;43(3):355-367. doi: 10.1007/s13318-017-0447-5. Eur J Drug Metab Pharmacokinet. 2018. PMID: 29119333 Free PMC article.
-
Prediction of drug-drug interaction potential using physiologically based pharmacokinetic modeling.Arch Pharm Res. 2017 Dec;40(12):1356-1379. doi: 10.1007/s12272-017-0976-0. Epub 2017 Oct 27. Arch Pharm Res. 2017. PMID: 29079968 Review.
-
Pharmacokinetic and pharmacodynamic drug interactions with new oral anticoagulants: what do they mean for patients with atrial fibrillation?Ann Pharmacother. 2013 Nov;47(11):1478-87. doi: 10.1177/1060028013504741. Epub 2013 Oct 9. Ann Pharmacother. 2013. PMID: 24259602 Review.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. Erratum in Lancet 2019, 393, e44. - DOI - PMC - PubMed
-
- Mamas M.A., Sperrin M., Watson M.C., Coutts A., Wilde K., Burton C., Kadam U.T., Kwok C.S., Clark A.B., Murchie P., et al. Do patients have worse outcomes in heart failure than in cancer? A primary care-based cohort study with 10-year follow-up in Scotland. Eur. J. Heart Fail. 2017;19:1095–1104. doi: 10.1002/ejhf.822. - DOI - PubMed
-
- McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M., Burri H., Butler J., Čelutkienė J., Chioncel O., et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021;42:3599–3726. doi: 10.1093/eurheartj/ehab368. Erratum in Eur. Heart J. 2021, 42, 4901. - DOI - PubMed
-
- Heidenreich P.A., Bozkurt B., Aguilar D., Allen L.A., Byun J.J., Colvin M.M., Deswal A., Drazner M.H., Dunlay S.M., Evers L.R., et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e876–e894. doi: 10.1161/CIR.0000000000001062. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
