

Lipoprotein(a) and Risk of Incident Atherosclerotic Cardiovascular Disease: Impact of High-Sensitivity C-Reactive Protein and Risk Variability Among Human Clinical Subgroups
- PMID: 40284189
- PMCID: PMC12030245
- DOI: 10.3390/nu17081324
Lipoprotein(a) and Risk of Incident Atherosclerotic Cardiovascular Disease: Impact of High-Sensitivity C-Reactive Protein and Risk Variability Among Human Clinical Subgroups
Abstract
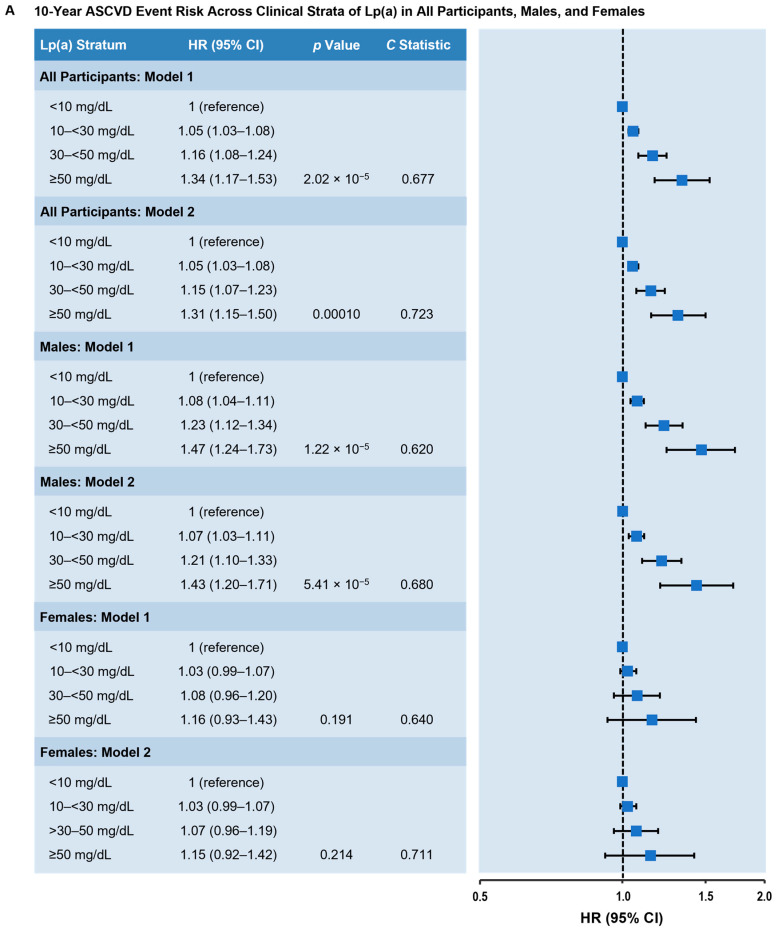
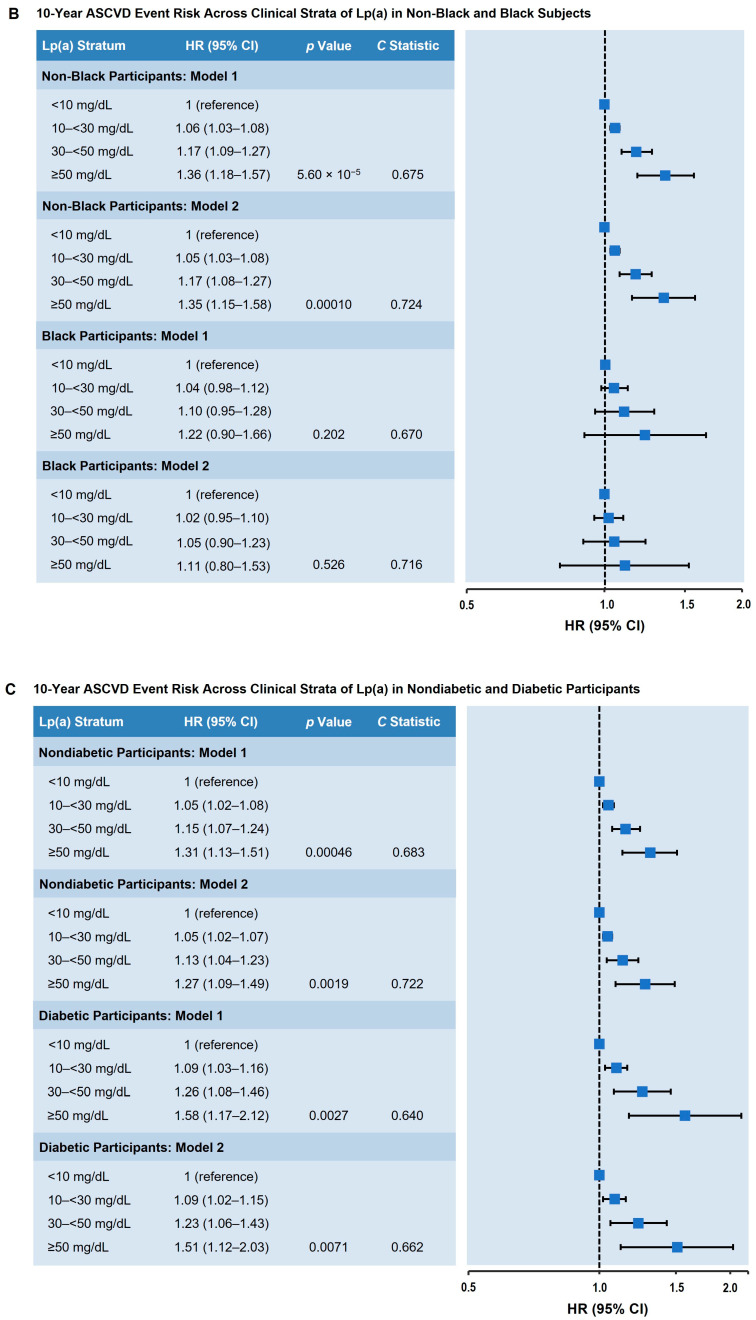
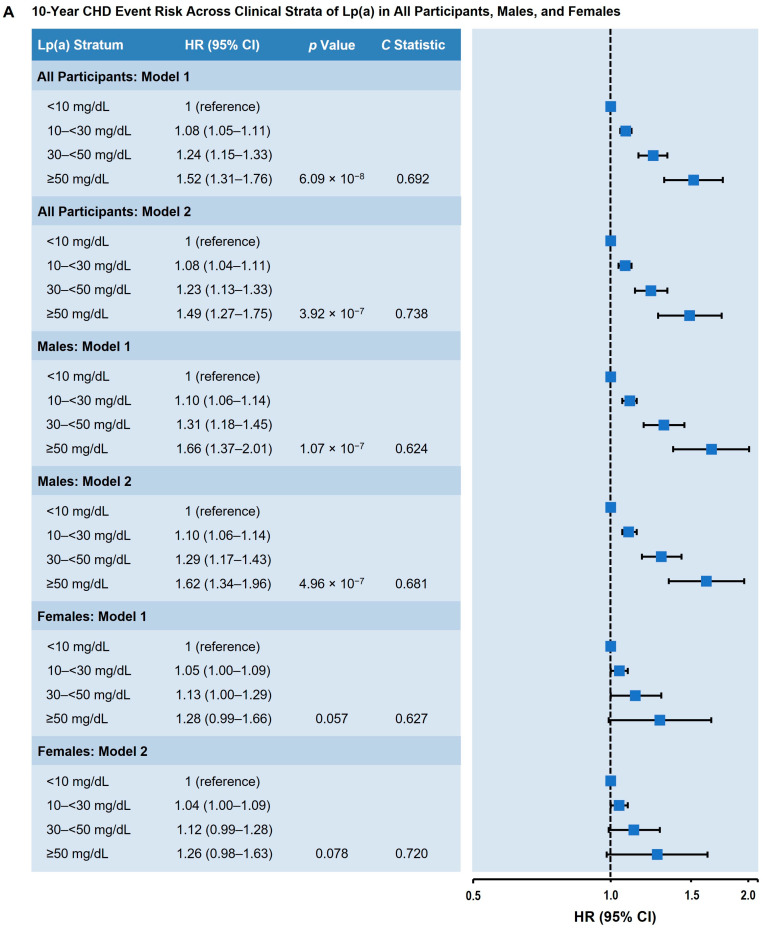
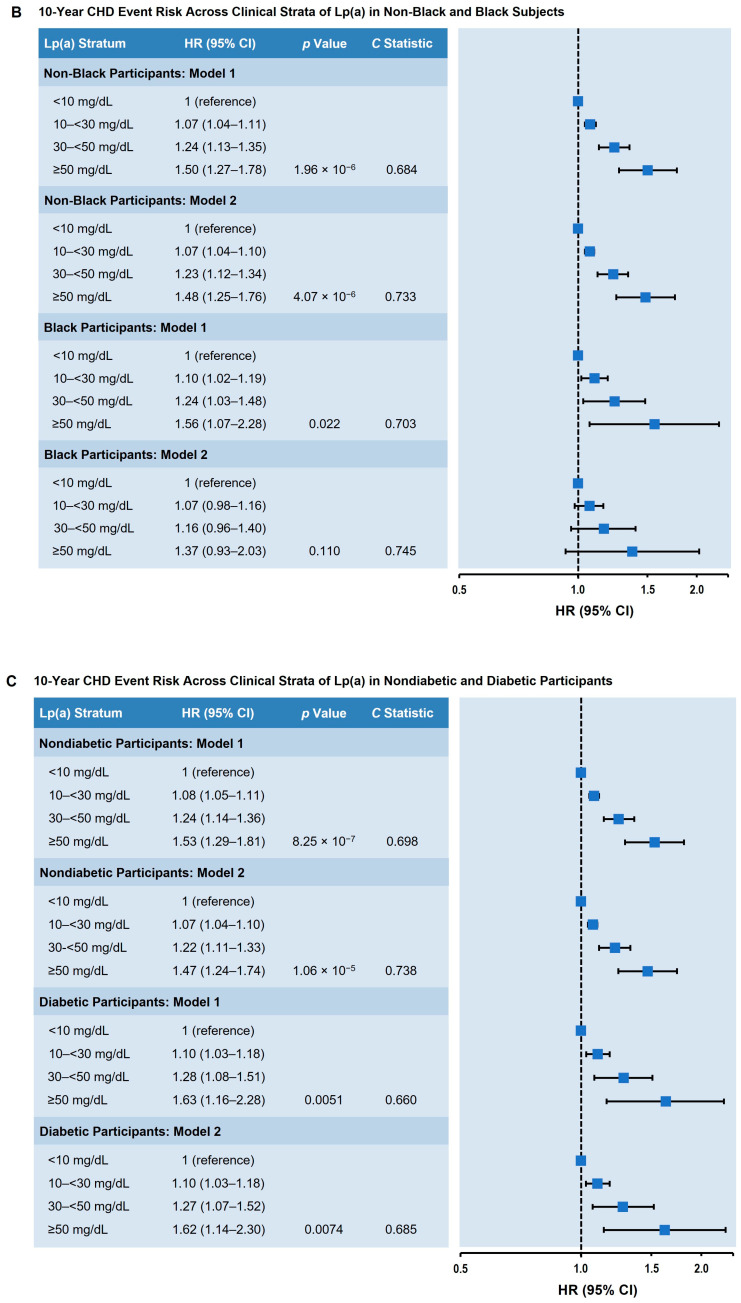
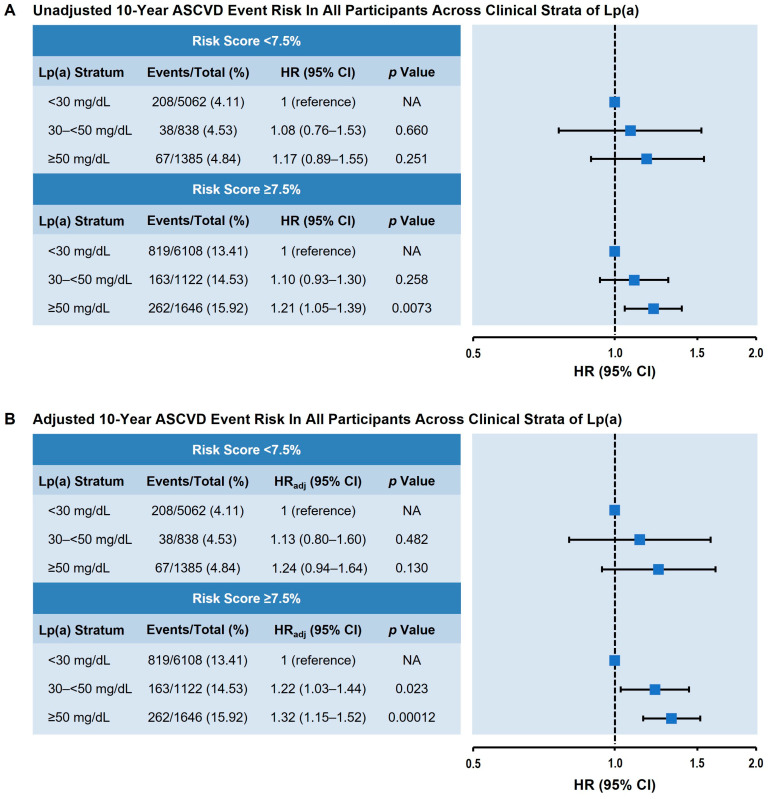
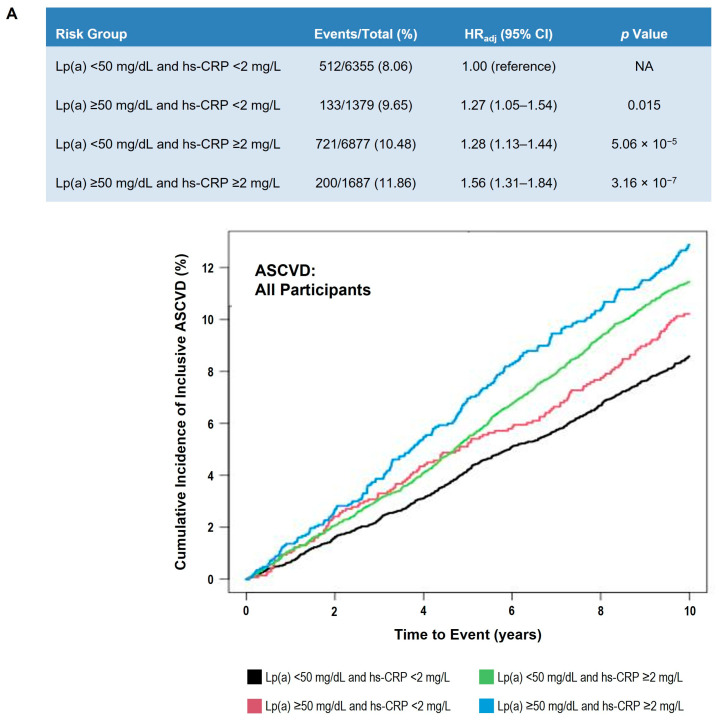
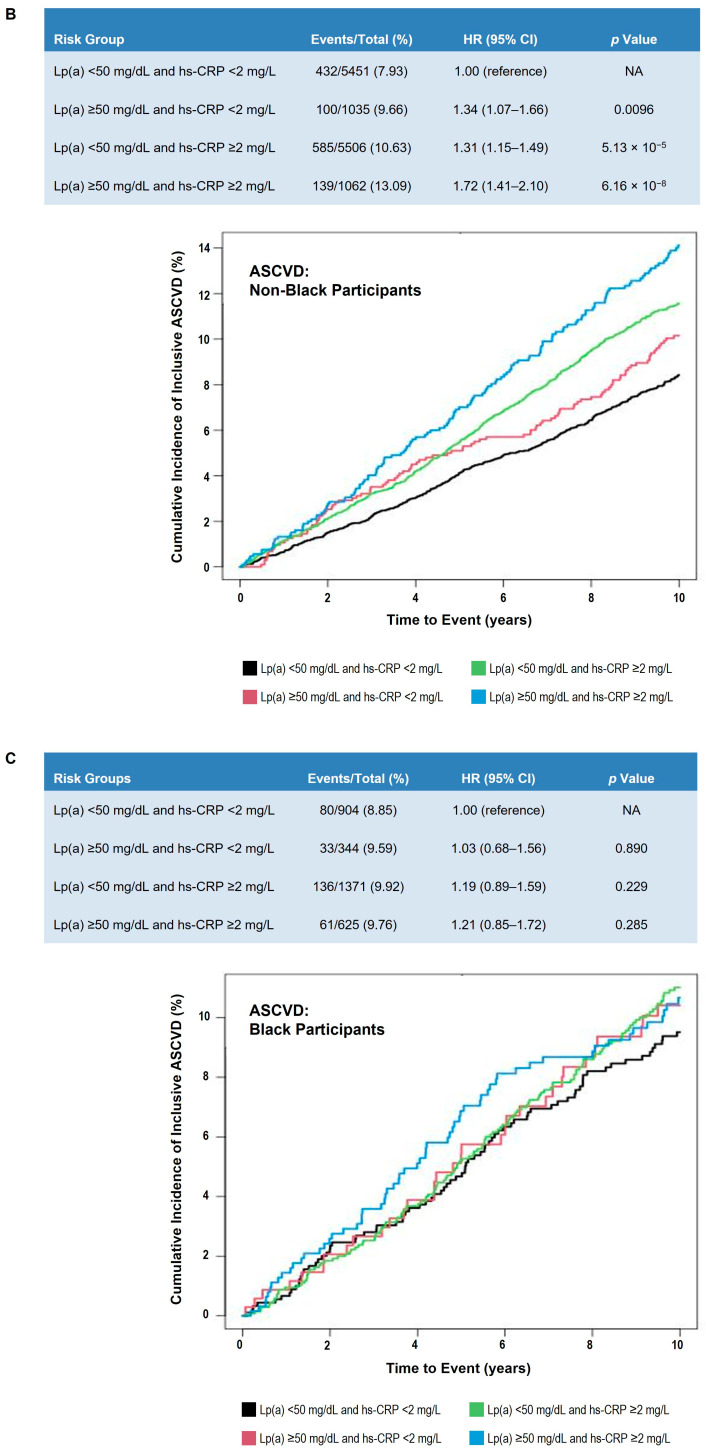
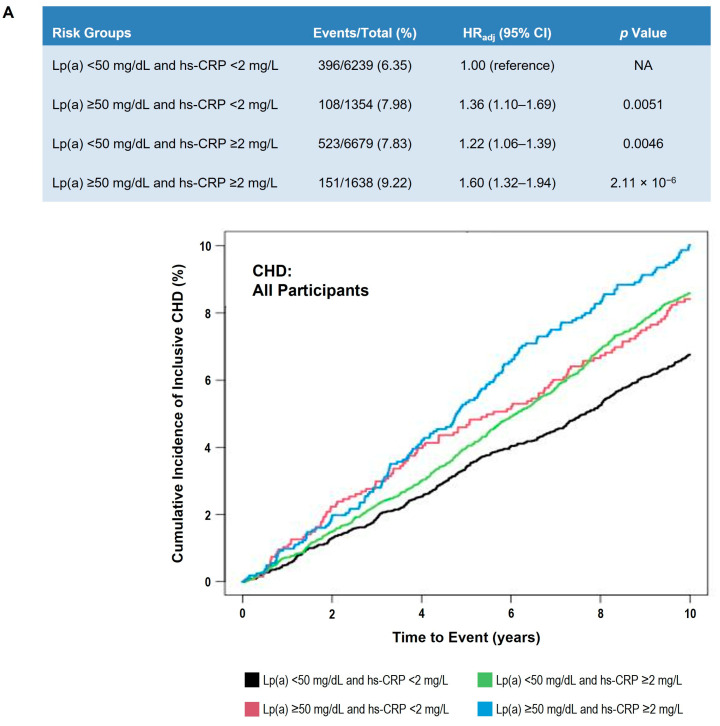
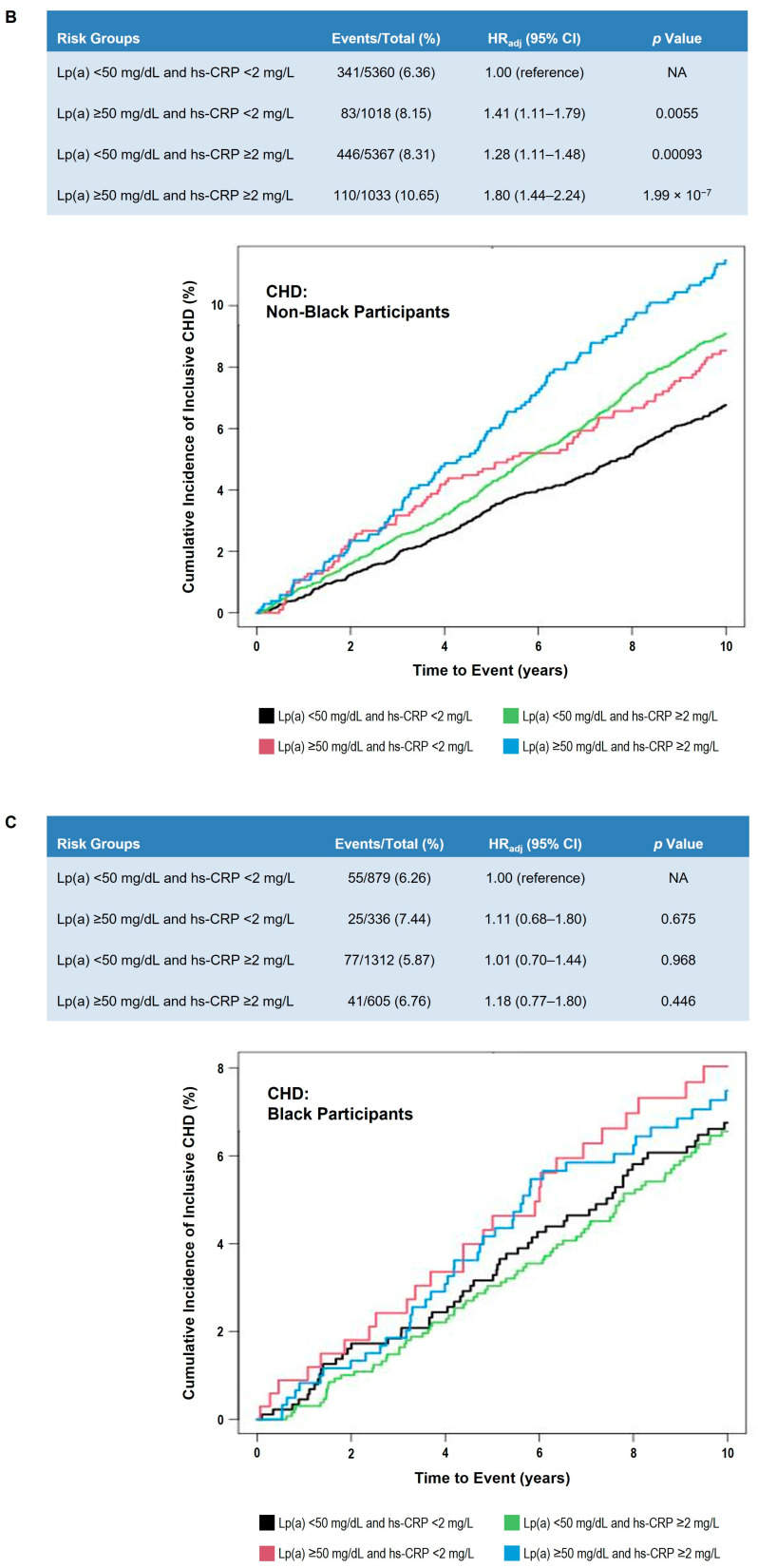
Background/Objectives: Elevated lipoprotein(a) [Lp(a)] is associated with increased incidence of atherosclerotic cardiovascular disease (ASCVD). We aimed to assess the utility of Lp(a) as an ASCVD risk-enhancing factor, as recommended by the 2019 ACC/AHA guidelines on ASCVD primary prevention, and to determine whether C-reactive protein (CRP) modifies the association of elevated Lp(a) with ASCVD risk. Methods: Lp(a), high sensitivity CRP (hs-CRP), and other ASCVD risk factors, including blood lipids, blood pressure, diabetes status, body weight and height, and smoking, were measured in 15,933 participants (median age 61.7 years with 25th-75th percentiles 57-68 years, 56.7% female, 19.7% Black, free of ASCVD at baseline) in the Atherosclerosis Risk in Communities Study, Framingham Offspring Study, and Multi-Ethnic Study of Atherosclerosis. Participants were followed for 10 years for incident ASCVD (coronary heart disease (CHD) or stroke) and CHD (including angioplasty and/or coronary artery bypass but minus stroke). These endpoints occurred in 9.7% and 7.4% of subjects, respectively. Results: Compared with the lowest Lp(a) category (<10 mg/dL), the highest Lp(a) category (≥50 mg/dL) carried a significantly increased incidence of ASCVD (hazard ratio [HR] = 1.31; 95% confidence interval [CI] 1.15-1.50; p < 0.001) and CHD (HR = 1.49; 95%CI 1.27-1.75; p < 0.001). The association of elevated Lp(a) with incident ASCVD was stronger in males and non-Black individuals and was independent of diabetes status. Lp(a) levels ≥ 50 mg/dL predicted the 10-year ASCVD risk for those at intermediate risk (≥7.5%, HR = 1.32; 95%CI 1.15-1.52; p < 0.001). There was a significant interaction between Lp(a) and hs-CRP; individuals with concomitant elevated levels of Lp(a) and hs-CRP had the highest ASCVD risk. Conclusions: Elevated Lp(a) levels were associated with increased ASCVD risk, particularly in individuals with concomitantly elevated hs-CRP levels and those at intermediate 10-year ASCVD risk.
Keywords: CRP; Lp(a); cardiovascular disease; diabetes.
Conflict of interest statement
R.C.H. has received research grants (to his institution) from Denka Corporation (Tokyo, Japan). R.C.H. and C.M.B. are consultants for Denka Seiken (Tokyo, Japan). M.R.D. is an employee of Boston Heart Diagnostics Corporation. None of the other authors have any relevant relationships or conflicts of interest to disclose.
Figures
References
-
- Burgess S., Ference B.A., Staley J.R., Freitag D.F., Mason A.M., Nielsen S.F., Willeit P., Young R., Surendran P., Karthikeyan S., et al. Association of LPA variants with risk of coronary disease and the implications for lipoprotein(a)-lowering therapies: A Mendelian randomization analysis. JAMA Cardiol. 2018;3:619–627. doi: 10.1001/jamacardio.2018.1470. - DOI - PMC - PubMed
-
- Emerging Risk Factors Collaboration. Erqou S., Kaptoge S., Perry P.L., Di Angelantonio E., Thompson A., White I.R., Marcovina S.M., Collins R., Thompson S.G., et al. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302:412–423. doi: 10.1001/jama.2009.1063. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
