

Overweight, Obesity, and Depression in Multimorbid Older Adults: Prevalence, Diagnostic Agreement, and Associated Factors in Primary Care-Results from a Multicenter Observational Study
- PMID: 40284257
- PMCID: PMC12030450
- DOI: 10.3390/nu17081394
Overweight, Obesity, and Depression in Multimorbid Older Adults: Prevalence, Diagnostic Agreement, and Associated Factors in Primary Care-Results from a Multicenter Observational Study
Abstract
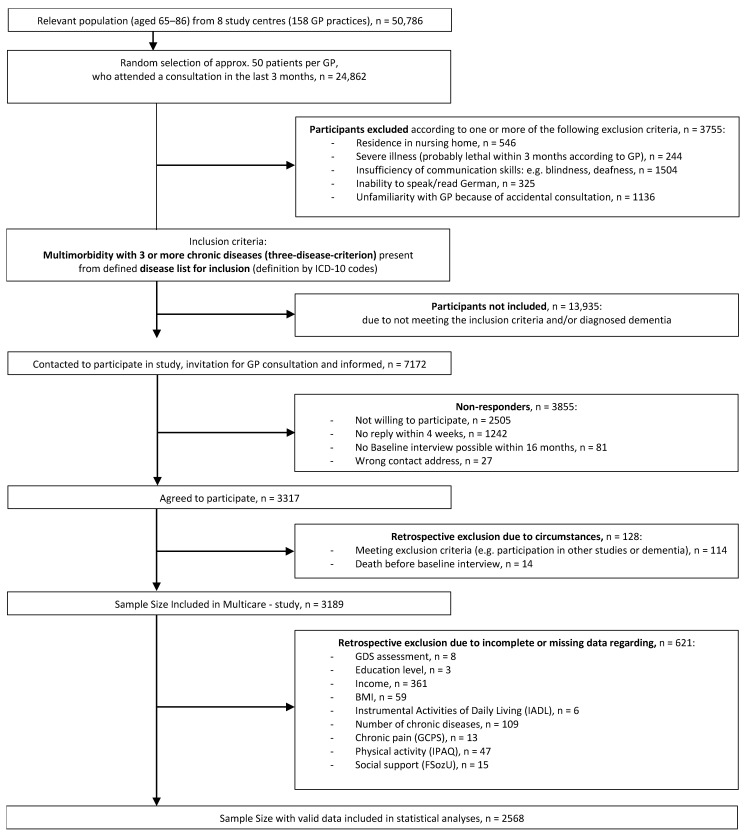
Background/Objectives: Obesity and depression, in conjunction with multimorbidity, are interconnected conditions increasingly managed in general practitioner (GP) settings, yet these associations remain insufficiently studied in older patients. This study investigates the prevalence of depression across different body mass index (BMI) classes and includes age and gender differences in multimorbid older patients, offering a novel perspective on subgroup-specific patterns. Further the agreement between GP depression diagnoses and the Geriatric Depression Scale (GDS) is studied and patient-specific factors that may affect the agreement are explored, aiming to improve future diagnostics for vulnerable subgroups. Methods: Data were provided by the baseline assessment of the MultiCare Study, a prospective multicenter observational cohort of multimorbid patients aged 65+ years recruited from 158 GP practices across eight study centers in Germany. Data from 2568 study participants were analyzed based on GP-coded International Classification of Diseases (ICD) diagnoses, structured GP questionnaires, and patient questionnaires. Assessments included data on the BMI and depression (15 item version of the GDS). Agreement between GP diagnoses of depression and GDS assessment was measured using Cohen's kappa. Four logistic regression models were used to examine the effects of patient-specific factors on the agreement of depression diagnosis (match or mismatch). Results: GPs diagnosed depression in 17.3% of cases, compared to the detection of depressive symptoms in 12.4% of the patients by GDS (cut-off ≥ 6 points). The highest prevalence rates were observed in patients with obesity class III (25.0% by GP; 21.7% by GDS). Women were significantly more likely to receive a depression diagnosis by a GP across most BMI classes (except obesity classes II and III). The detection of depressive symptoms by GDS was significantly more prevalent in older multimorbid obese patients (≥75 years), except for patients with obesity class III. The overall agreement between GP diagnosis and GDS assessment was weak (κ = 0.156, p < 0.001). The highest agreement was found for people with obesity class III (κ = 0.256, p < 0.05). Factors associated with a True Positive depression diagnosis (match by both GDS and GP) were female gender (odds ratio (OR) = 1.83, p < 0.05), widowhood (OR = 2.43, p < 0.01), limited daily living skills (OR = 3.14, p < 0.001), and a higher level of education (OR = 2.48, p < 0.01). A significantly lower likelihood of a False Negative depression diagnosis was found for patients with obesity class III. Conclusions: This study highlights the significant prevalence of depression among multimorbid older adults across different BMI classes, particularly in those with obesity class III. The weak diagnostic agreement between GP diagnosis and GDS assessment suggests a need for improved diagnostic practices in primary care. Implementing standardized screening tools and fostering collaboration with mental health specialists could enhance the identification and management of depression in this vulnerable population.
Keywords: Geriatric Depression Scale; body mass index; depression; late life; multimorbidity; obesity; primary care.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures


Similar articles
-
A comparison of GP and GDS diagnosis of depression in late life among multimorbid patients - results of the MultiCare study.J Affect Disord. 2014 Oct;168:276-83. doi: 10.1016/j.jad.2014.06.020. Epub 2014 Jun 18. J Affect Disord. 2014. PMID: 25080391
-
Agreement between self-reported and general practitioner-reported chronic conditions among multimorbid patients in primary care - results of the MultiCare Cohort Study.BMC Fam Pract. 2014 Mar 1;15:39. doi: 10.1186/1471-2296-15-39. BMC Fam Pract. 2014. PMID: 24580758 Free PMC article.
-
The influence of age, gender and socio-economic status on multimorbidity patterns in primary care. First results from the multicare cohort study.BMC Health Serv Res. 2012 Apr 3;12:89. doi: 10.1186/1472-6963-12-89. BMC Health Serv Res. 2012. PMID: 22471952 Free PMC article.
-
Accuracy of the Geriatric Depression Scale (GDS)-4 and GDS-5 for the screening of depression among older adults: A systematic review and meta-analysis.PLoS One. 2021 Jul 1;16(7):e0253899. doi: 10.1371/journal.pone.0253899. eCollection 2021. PLoS One. 2021. PMID: 34197527 Free PMC article.
-
Screening for depression and anxiety among older Chinese immigrants living in Western countries: The use of the Geriatric Depression Scale (GDS) and the Geriatric Anxiety Inventory (GAI).Asia Pac Psychiatry. 2016 Mar;8(1):32-43. doi: 10.1111/appy.12191. Epub 2015 May 22. Asia Pac Psychiatry. 2016. PMID: 26010903 Review.
References
-
- World Health Organization . MhGAP: Mental Health Gap Action Programme: Scaling up Care for Mental, Neurological, and Substance Use Disorders. World Health Organization; Geneva, Switzerland: 2008. - PubMed
-
- World Health Organization, editor. Mental Health Atlas 2017. World Health Organization; Geneva, Switzerland: 2018.
-
- World Health Organization, editor. Global Strategy on Diet, Physical Activity and Health. World Health Organization; Geneva, Switzerland: 2004.
-
- Bentham J., Di Cesare M., Bilano V. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128·9 Million Children, Adolescents, and Adults. Lancet. 2017;390:2627. doi: 10.1016/S0140-6736(17)32129-3. - DOI - PMC - PubMed
-
- World Health Organization Obesity and Overweight. [(accessed on 21 February 2025)]; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
