

Effects of parental autoimmune diseases on type 1 diabetes in offspring can be partially explained by HLA and non-HLA polymorphisms
- PMID: 40286789
- PMCID: PMC12230240
- DOI: 10.1016/j.xgen.2025.100854
Effects of parental autoimmune diseases on type 1 diabetes in offspring can be partially explained by HLA and non-HLA polymorphisms
Abstract
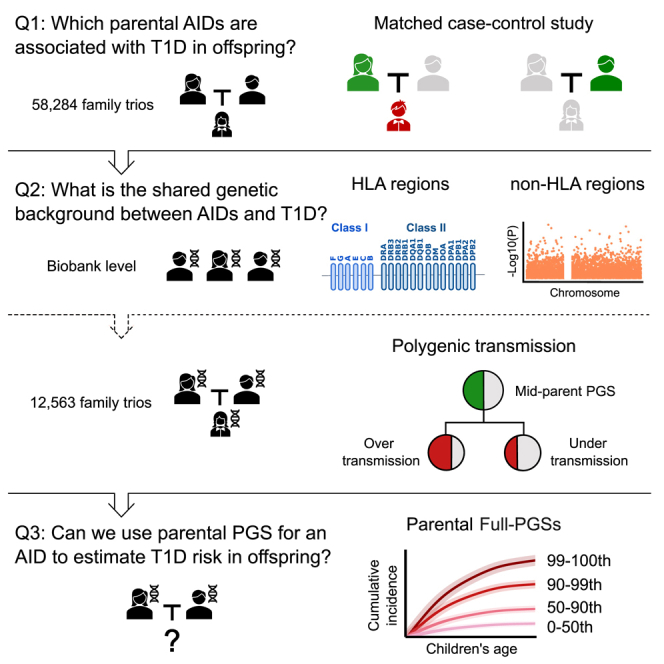
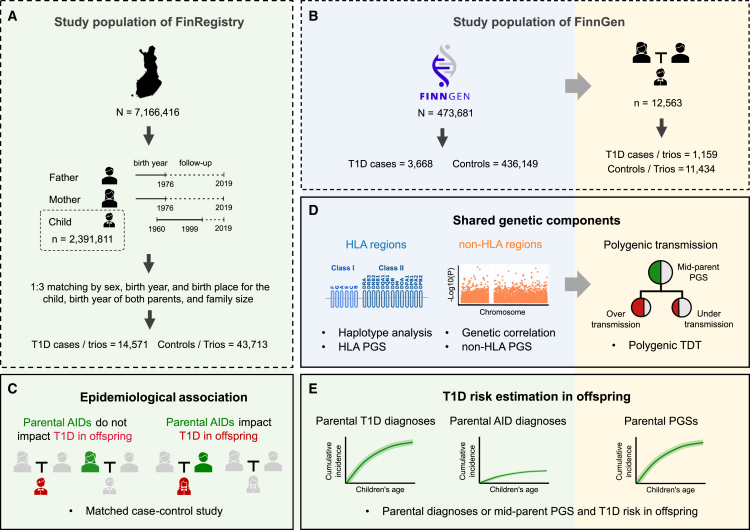
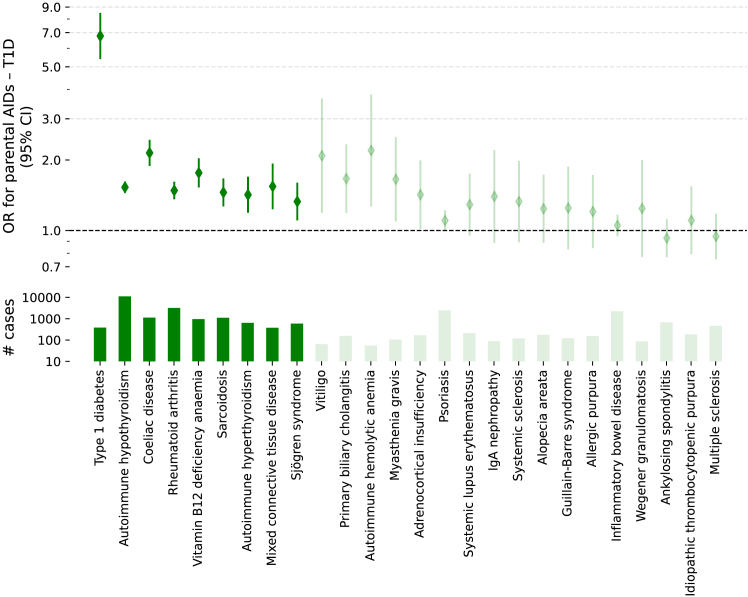
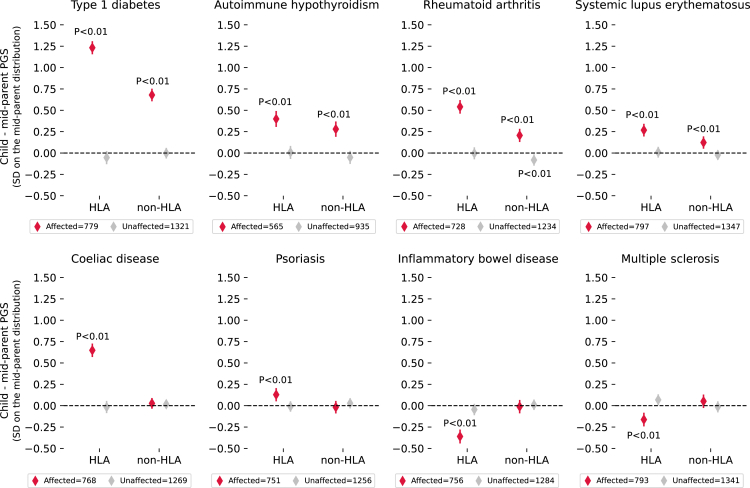
Type 1 diabetes (T1D) and other autoimmune diseases (AIDs) often co-occur in families. Leveraging data from 58,284 family trios in Finnish nationwide registers (FinRegistry), we identified that, of 50 parental AIDs examined, 15 were associated with an increased T1D risk in offspring. These identified epidemiological associations were further assessed in 470,000 genotyped Finns from the FinnGen study through comprehensive genetic analyses, partitioned into human leukocyte antigen (HLA) and non-HLA variations. Using FinnGen's 12,563 trios, a within-family polygenic transmission analysis demonstrated that the aggregation of many parental AIDs with offspring T1D can be partially explained by HLA and non-HLA polymorphisms in a disease-dependent manner. We therefore proposed a parental polygenic score (PGS), incorporating both HLA and non-HLA polymorphisms, to characterize the cumulative risk pattern of T1D in offspring. This raises an intriguing possibility of using parental PGS, in conjunction with clinical diagnoses, to inform individuals about T1D risk in their offspring.
Keywords: HLA; autoimmune disease; celiac disease; family history; genetic correlation; major histocompatibility complex; multi-trait PRS; polygenic risk score; polygenic transmission disequilibrium test; rheumatoid arthritis; type 1 diabetes.
Copyright © 2025 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests A.G. is the founder of Real World Genetics. R.O. holds a UK Medical Research Council Institutional Confidence in Concept grant to develop a 10 SNP biochip T1D genetic test in collaboration with Randox.
Figures


References
-
- Kavvoura F.K., Ioannidis J.P.A. CTLA-4 Gene Polymorphisms and Susceptibility to Type 1 Diabetes Mellitus: A HuGE Review and Meta-Analysis. Am. J. Epidemiol. 2005;162:3–16. - PubMed
-
- Knip M., Veijola R., Virtanen S.M., Hyöty H., Vaarala O., Åkerblom H.K. Environmental Triggers and Determinants of Type 1 Diabetes. Diabetes. 2005;54:S125–S136. - PubMed
-
- Gregory G.A., Robinson T.I.G., Linklater S.E., Wang F., Colagiuri S., De Beaufort C., Donaghue K.C., Magliano D.J., Maniam J., Orchard T.J., et al. Global incidence, prevalence, and mortality of type 1 diabetes in 2021 with projection to 2040: a modelling study. Lancet Diabetes Endocrinol. 2022;10:741–760. - PubMed
-
- Hormazábal-Aguayo I., Ezzatvar Y., Huerta-Uribe N., Ramírez-Vélez R., Izquierdo M., García-Hermoso A. Incidence of type 1 diabetes mellitus in children and adolescents under 20 years of age across 55 countries from 2000 to 2022: A systematic review with meta-analysis. Diabetes Metabolism Res. 2024;40 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
