

TLK1 as a therapeutic target in TMZ resistant glioblastoma using small molecule inhibitor
- PMID: 40287404
- PMCID: PMC12033314
- DOI: 10.1038/s41598-025-86599-3
TLK1 as a therapeutic target in TMZ resistant glioblastoma using small molecule inhibitor
Abstract
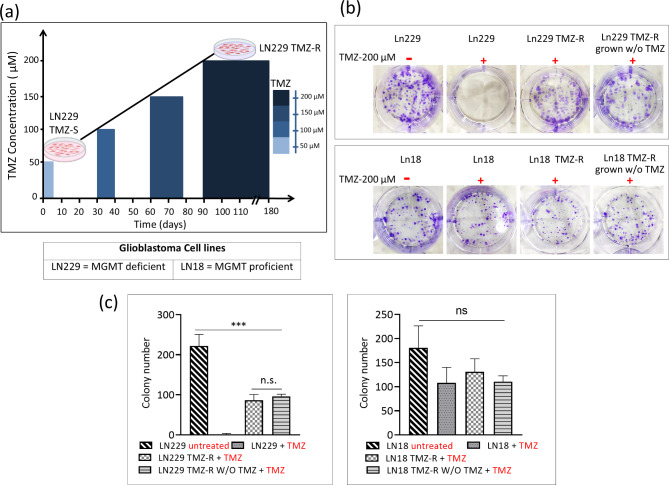
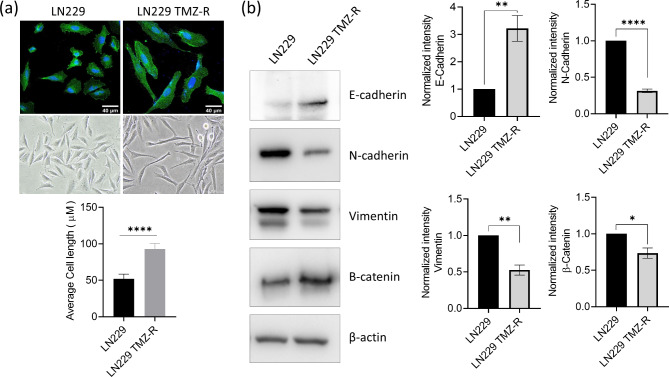
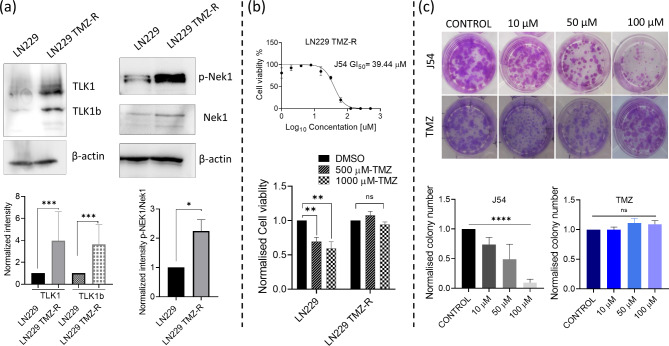
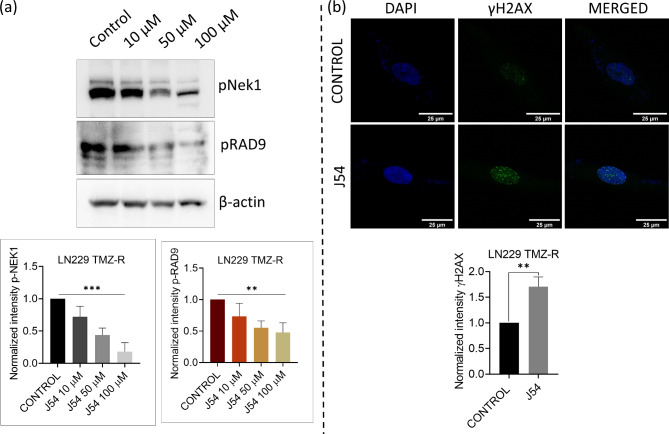
The acquired resistance to existing therapies poses a grave concern in achieving successful therapeutic outcomes. Temozolomide (TMZ), a widely used alkylating chemotherapeutic in Glioblastoma therapy, often encounters resistance, necessitating the investigation of the underlying mechanisms of TMZ-acquired resistance. To study TMZ resistance, a cell-based model system was generated by intermittently exposing glioblastoma cells to increasing concentrations and time of TMZ over six months. The survival response of cells at higher concentrations confirmed TMZ-resistant cells, which exhibited a phenotypic shift toward a mesenchymal-like state, with decreased epithelial traits, indicating mesenchymal-epithelial transition (MET). This transition likely facilitates the stabilization and clonal growth of TMZ-resistant cells. Subsequent analysis revealed elevated expression of TLK1, a DNA repair protein, thus reinforcing its potential involvement in mechanisms associated with acquired resistance. To explore the therapeutic aspect of TLK1 inhibition, we utilized an in-house developed TLK1 inhibitor, J54. The inhibition of TLK1 in TMZ-resistant cells enhanced cytotoxicity, indicating TLK1 as a potential target to combat TMZ resistance. Moreover, TLK1 inhibition reduced cell migration and invasion, implying its role in promoting metastasis. In conclusion, our study sheds light on the role of TLK1 in the context of TMZ resistance, highlighting its potential as a valuable target for therapeutic intervention.
Keywords: Blood-brain-barrier; DNA damage response; Glioblastoma; Phenothiazine; Temozolomide; Tousled-like kinase-1.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
A novel approach to investigate the combinatorial effects of TLK1 (Tousled-Like Kinase1) inhibitors with Temozolomide for glioblastoma therapy.Bioorg Chem. 2024 Oct;151:107643. doi: 10.1016/j.bioorg.2024.107643. Epub 2024 Jul 14. Bioorg Chem. 2024. PMID: 39029318
-
Alterations in Cell Motility, Proliferation, and Metabolism in Novel Models of Acquired Temozolomide Resistant Glioblastoma.Sci Rep. 2018 May 8;8(1):7222. doi: 10.1038/s41598-018-25588-1. Sci Rep. 2018. PMID: 29740146 Free PMC article.
-
20(S)-ginsenoside-Rg3 reverses temozolomide resistance and restrains epithelial-mesenchymal transition progression in glioblastoma.Cancer Sci. 2019 Jan;110(1):389-400. doi: 10.1111/cas.13881. Epub 2018 Dec 14. Cancer Sci. 2019. PMID: 30431207 Free PMC article.
-
Involvement of Intracellular Cholesterol in Temozolomide-Induced Glioblastoma Cell Death.Neurol Med Chir (Tokyo). 2018 Jul 15;58(7):296-302. doi: 10.2176/nmc.ra.2018-0040. Epub 2018 Jun 13. Neurol Med Chir (Tokyo). 2018. PMID: 29899179 Free PMC article. Review.
-
Dysregulated lipid metabolism in TMZ-resistant glioblastoma: pathways, proteins, metabolites and therapeutic opportunities.Lipids Health Dis. 2023 Aug 3;22(1):114. doi: 10.1186/s12944-023-01881-5. Lipids Health Dis. 2023. PMID: 37537607 Free PMC article. Review.
References
-
- Stupp, R. et al. Radiotherapy plus concomitant and Adjuvant Temozolomide for Glioblastoma. N Engl. J. Med.352 (10), 987–996 (2005). - PubMed
-
- Zhang, J., Stevens, F. G., Bradshaw, M. D. & Temozolomide, T. Mechanisms of action, repair and resistance. Curr. Mol. Pharmacol.5 (1), 102–114 (2012). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
